

Early bolus epinephrine administration during pediatric cardiopulmonary resuscitation for bradycardia with poor perfusion: an ICU-resuscitation study
- PMID: 39010134
- PMCID: PMC11251231
- DOI: 10.1186/s13054-024-05018-7
Early bolus epinephrine administration during pediatric cardiopulmonary resuscitation for bradycardia with poor perfusion: an ICU-resuscitation study
Abstract
Background: Half of pediatric in-hospital cardiopulmonary resuscitation (CPR) events have an initial rhythm of non-pulseless bradycardia with poor perfusion. Our study objectives were to leverage granular data from the ICU-RESUScitation (ICU-RESUS) trial to: (1) determine the association of early epinephrine administration with survival outcomes in children receiving CPR for bradycardia with poor perfusion; and (2) describe the incidence and time course of the development of pulselessness.
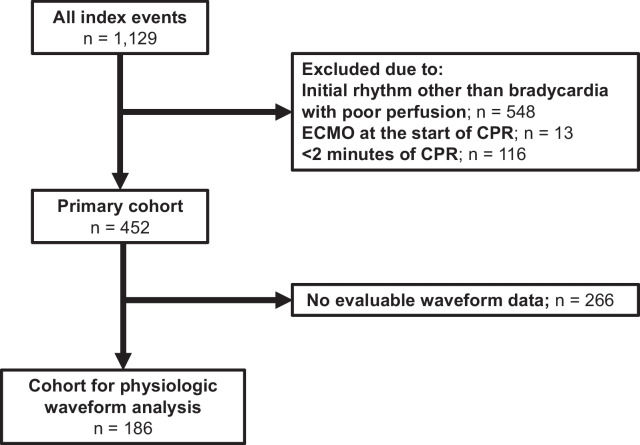
Methods: Prespecified secondary analysis of ICU-RESUS, a multicenter cluster randomized trial of children (< 19 years) receiving CPR in 18 intensive care units in the United States. Index events (October 2016-March 2021) lasting ≥ 2 min with a documented initial rhythm of bradycardia with poor perfusion were included. Associations between early epinephrine (first 2 min of CPR) and outcomes were evaluated with Poisson multivariable regression controlling for a priori pre-arrest characteristics. Among patients with arterial lines, intra-arrest blood pressure waveforms were reviewed to determine presence of a pulse during CPR interruptions. The temporal nature of progression to pulselessness was described and outcomes were compared between patients according to subsequent pulselessness status.
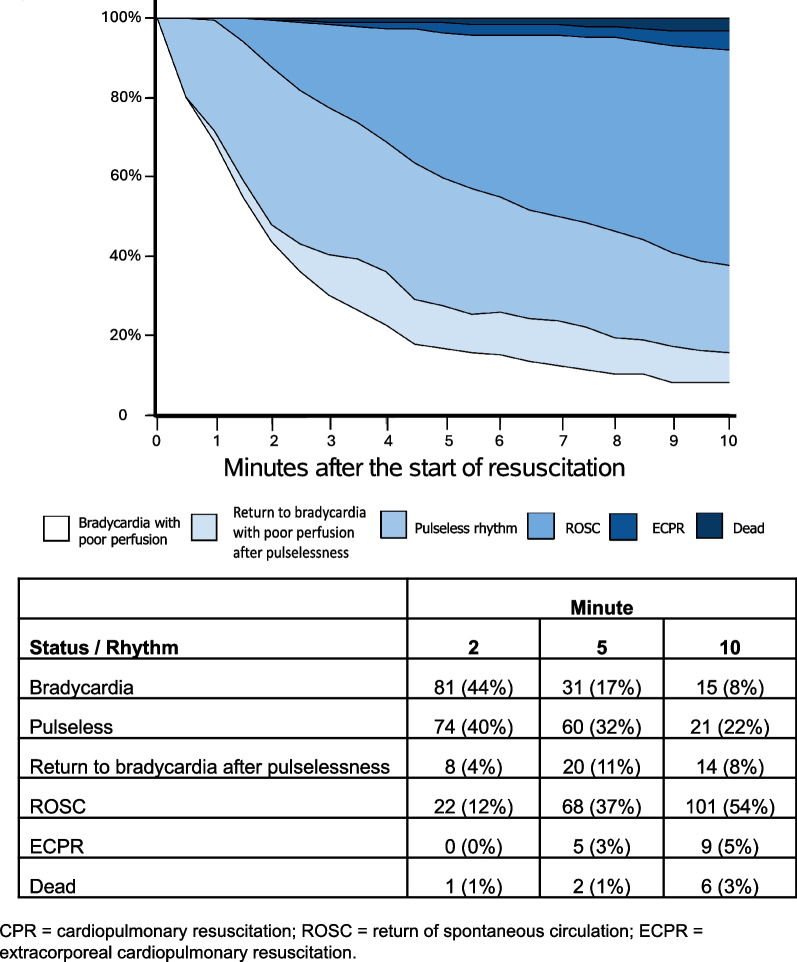
Results: Of 452 eligible subjects, 322 (71%) received early epinephrine. The early epinephrine group had higher pre-arrest severity of illness and vasoactive-inotrope scores. Early epinephrine was not associated with survival to discharge (aRR 0.97, 95%CI 0.82, 1.14) or survival with favorable neurologic outcome (aRR 0.99, 95%CI 0.82, 1.18). Among 186 patients with invasive blood pressure waveforms, 118 (63%) had at least 1 period of pulselessness during the first 10 min of CPR; 86 (46%) by 2 min and 100 (54%) by 3 min. Sustained return of spontaneous circulation was highest after bradycardia with poor perfusion (84%) compared to bradycardia with poor perfusion progressing to pulselessness (43%) and bradycardia with poor perfusion progressing to pulselessness followed by return to bradycardia with poor perfusion (62%) (p < 0.001).
Conclusions: In this cohort of pediatric CPR events with an initial rhythm of bradycardia with poor perfusion, we failed to identify an association between early bolus epinephrine and outcomes when controlling for illness severity. Most children receiving CPR for bradycardia with poor perfusion developed subsequent pulselessness, 46% within 2 min of CPR onset.
Keywords: Bradycardia; Cardiopulmonary resuscitation; Epinephrine; Heart arrest; Hemodynamics; Pediatric intensive care units.
© 2024. The Author(s).
Conflict of interest statement
Drs. Reeder’s, Carcillo’s, Carpenter’s, Dean’s, Fink’s, Frazier’s, Friess’, Hall’s, Manga’s, Morgan’s, Mourani’s, Nadkarni’s, Naim’s, Palmer’s, Pollack’s, Wessel’s, Wolfe’s, Yates’, Zuppa’s, Sutton’s, and Meert’s institutions received funding from the National Institutes of Health (NIH). Drs. Reeder, Berg, Carcillo, Carpenter, Dean, Fink, Frazier, Friess, Hall, Horvat, Maa, McQuillen, Meert, Morgan, Mourani, Nadkarni, Naim, Pollack, Wessel, Wolfe, Yates, and Zuppa received support for article research from the NIH. Dr. Berg’s institution received funding from the National Institute of Child Health and Human Development (NICHD) Collaborative Pediatric Critical Care Research Network grant and the National Heart, Lung, and Blood Institute (NHLBI) ICU-RESUS trial grant. Dr. Fink’s institution received funding from the Neurocritical Care Society; she received funding from the American Board of Pediatrics and the Child Neurology Society. Dr. Friess received funding from an expert witness testimony. Dr. Hall received funding from Abbvie, La Jolla Pharmaceuticals, and Kiadis. Drs. Horvat, Maa, and McQuillen’s institutions received funding from the NICHD. Dr. Horvat’s institution received funding from the National Institute of Neurological Disorders and Stroke. Dr. Maa’s institution received funding from the NHLBI. Dr. Mourani disclosed the off-label product use of sodium bicarbonate. Dr. Pollack disclosed work for hire. Dr. Wolfe received funding from The Debriefing Academy and Zoll. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Topjian AA, Raymond TT, Atkins D, Chan M, Duff JP, Joyner BL, et al. Part 4: pediatric basic and advanced life support: 2020 american heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16_suppl_2):S469–S523. doi: 10.1161/CIR.0000000000000901. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UG1HD050096/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- U01HD049934/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- UG1HD049981/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- R01HL147616/HL/NHLBI NIH HHS/United States
- UG1HD083166/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- R01HL131544/HL/NHLBI NIH HHS/United States
- K23 HL148541/HL/NHLBI NIH HHS/United States
- UG1HD063108/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- UG1 HD083171/HD/NICHD NIH HHS/United States
- UG1HD083171/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- PL1 HD105462/HD/NICHD NIH HHS/United States
- UG1HD083170/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- UG1HD049983/National Institutes of Health Eunice Kennedy Shriver National Institute of Child Health and Human Development
- K23HL148541/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
