

Cardiovascular events in CML patients treated with Nilotinib: validation of the HFA-ICOS baseline risk score
- PMID: 39010172
- PMCID: PMC11247904
- DOI: 10.1186/s40959-024-00245-x
Cardiovascular events in CML patients treated with Nilotinib: validation of the HFA-ICOS baseline risk score
Abstract
Background: The therapeutic landscape of chronic myeloid leukaemia (CML) has been transformed by tyrosine kinase inhibitors (TKI). Nilotinib, showed higher rates of major molecular response than imatinib, however associated with higher cardiovascular (CV) toxicity. We sought to describe the CV events associated with nilotinib in a real-world population and assess the predictive value of the HFA-ICOS risk score.
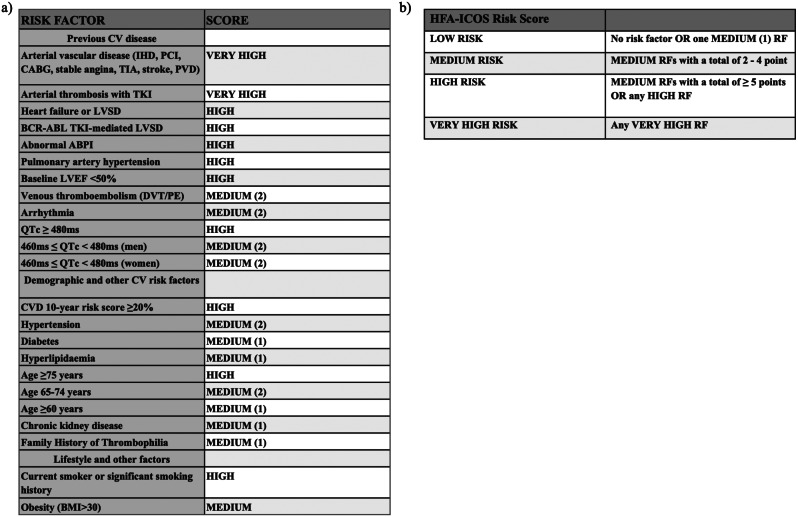
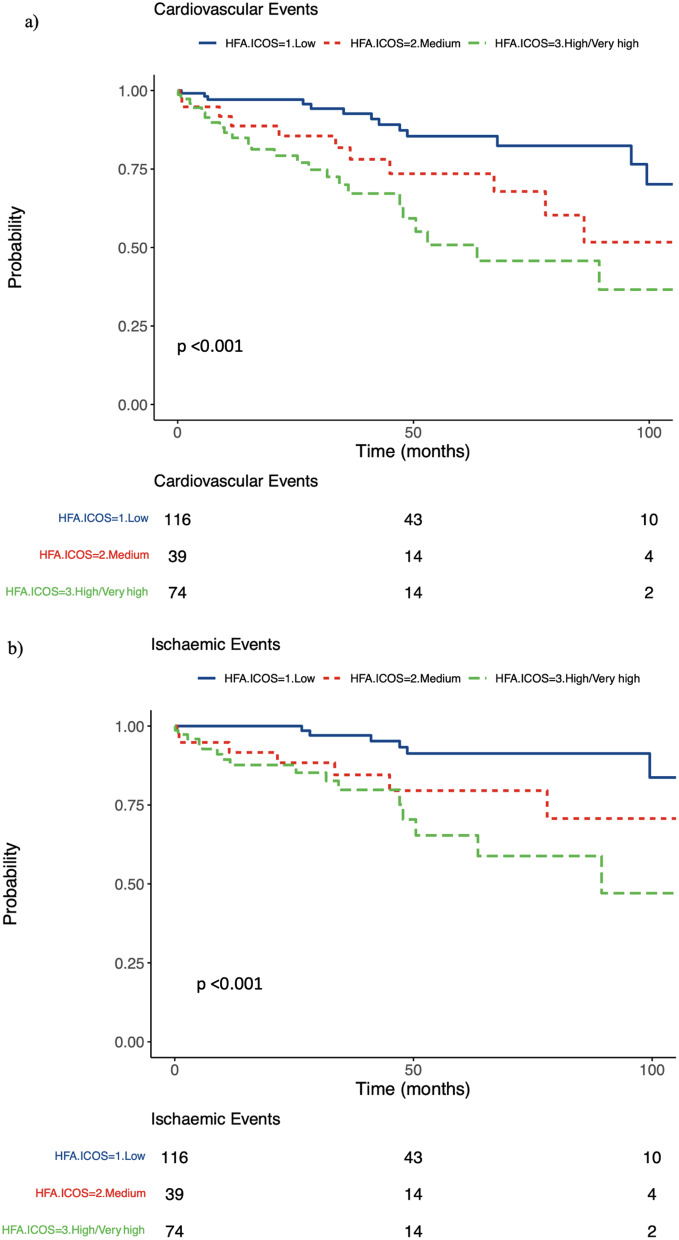
Methods: The HFA-ICOS baseline risk was calculated for patients with CML treated with nilotinib beween 2006 and 2021. The primary end point was the incidence of all CV events. The secondary end point was the incidence of ischaemic events. Survival analysis evaluated the risk (hazard ratio [HR]) of events stratified by baseline risk category, whilst on nilotinib therapy.
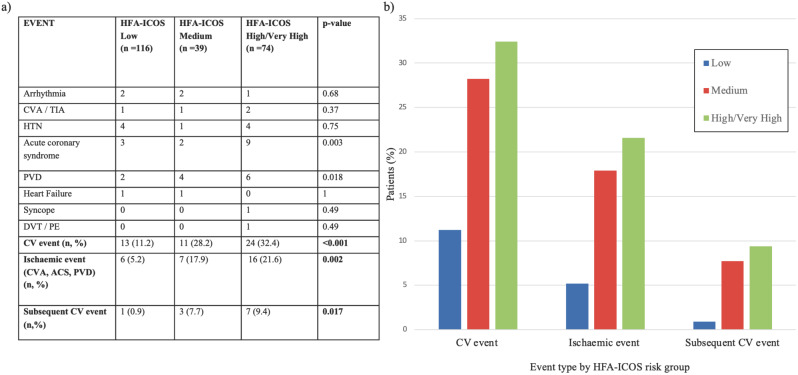
Results: Two hundred and twenty-nine eligible patients were included. The incidence of CV events was 20.9% (95% CI: 15.7-26.2%) following a median duration of treatment of 34.4 months. The secondary end point occurred in 12.7% (95% CI: 8.4-16.9%) of the population. Patients with higher HFA-ICOS baseline score had higher rates of CV events (low: 11.2%, medium: 28.2% [HR: 2.51, 95% CI: 1.17-5.66], high/very high: 32.4% [HR: 3.57, 95% CI: 1.77-7.20]) and ischaemic events (low: 5.20%, medium: 17.9% [HR: 2.19, 95% CI: 0.97-4.96], high/very high: 21.6% [HR: 3.9, 95% CI: 1.91-7.89]). In patients who did not have a CV event, the median total dose at last follow up or cessation of nilotinib therapy was lower when compared to the total daily median dose of nilotinib in patients who had a CV event (450 mg vs. 600 mg, p = 0.0074).
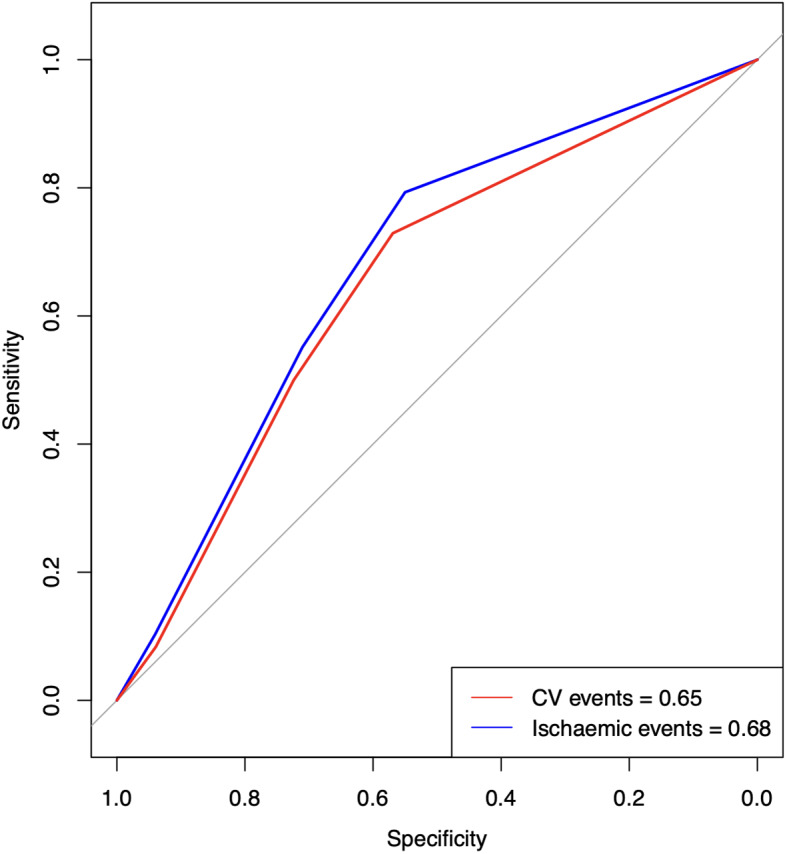
Conclusions: The HFA-ICOS risk stratification tool is an efficient discriminator at low, medium and high/very high risk of developing cardiovascular events, with an overall positive trend towards increasing cardiotoxicity rates with rising risk catergories. This study provides evidence to support the use of this predictive tool in nilotinib treated patients.
Keywords: CV toxicity; Chronic myeloid leukaemia; Nilotinib; Risk stratification; TKI.
© 2024. The Author(s).
Conflict of interest statement
ARL has received speaker, advisory board or consultancy fees and/or research grants from Janssens-Cilag Ltd, Astellas Pharma, Pfizer, Novartis, Servier, Astra Zeneca, Bristol Myers Squibb, GSK, Amgen, Takeda, Roche, Clinigen Group, Eli Lily, Eisai Ltd, Ferring Pharmaceuticals, Boehringer Ingelheim, Akcea Therapeutics, Myocardial Solutions, iOWNA Health and Heartfelt Technologies Ltd. MSA is funded by the Royal Brompton Hospital Charity. ARL is supported by the Fondation Leducq Network of Excellence in Cardio-Oncology and the Royal Brompton Cardio-Oncology Centre of Excellence is supported by the The Big Heart Foundation. The remaining authors have nothing to disclose.
Figures

References
LinkOut - more resources
Full Text Sources