

Projecting the clinical burden of chronic kidney disease at the patient level (Inside CKD): a microsimulation modelling study
- PMID: 39010981
- PMCID: PMC11247147
- DOI: 10.1016/j.eclinm.2024.102614
Projecting the clinical burden of chronic kidney disease at the patient level (Inside CKD): a microsimulation modelling study
Abstract
Background: Chronic kidney disease (CKD) is a global concern that presents significant challenges for disease management. Several factors drive CKD prevalence, including primary risk factors, such as type 2 diabetes and hypertension, and an ageing population. Inside CKD is an international initiative that aims to raise awareness of the substantial burden incurred by CKD.
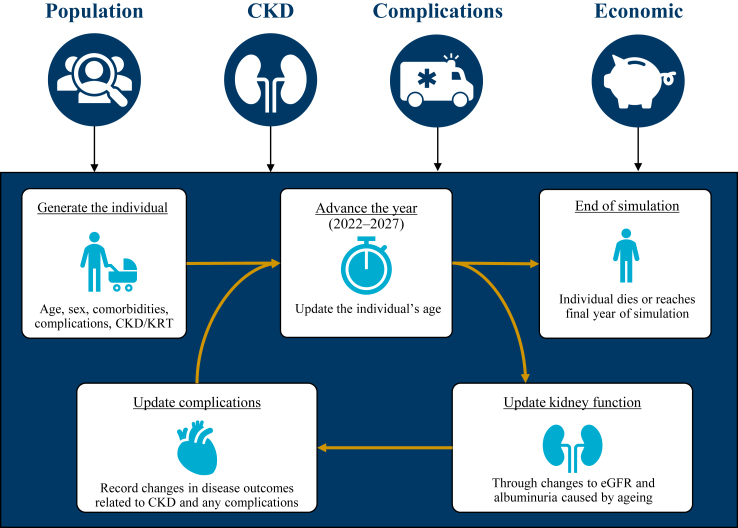
Methods: Using a peer-reviewed microsimulation method, the clinical burden of CKD was estimated from 2022 to 2027. Demographic data from the Americas, Europe, and Asia-Pacific/Middle East were used to generate virtual populations and to project the prevalence of CKD, kidney replacement therapy, associated cardiovascular complications, comorbid conditions, and all-cause mortality in the CKD population over the modelled time frame.
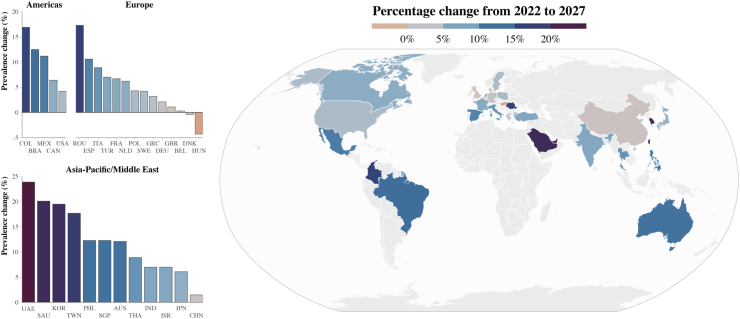
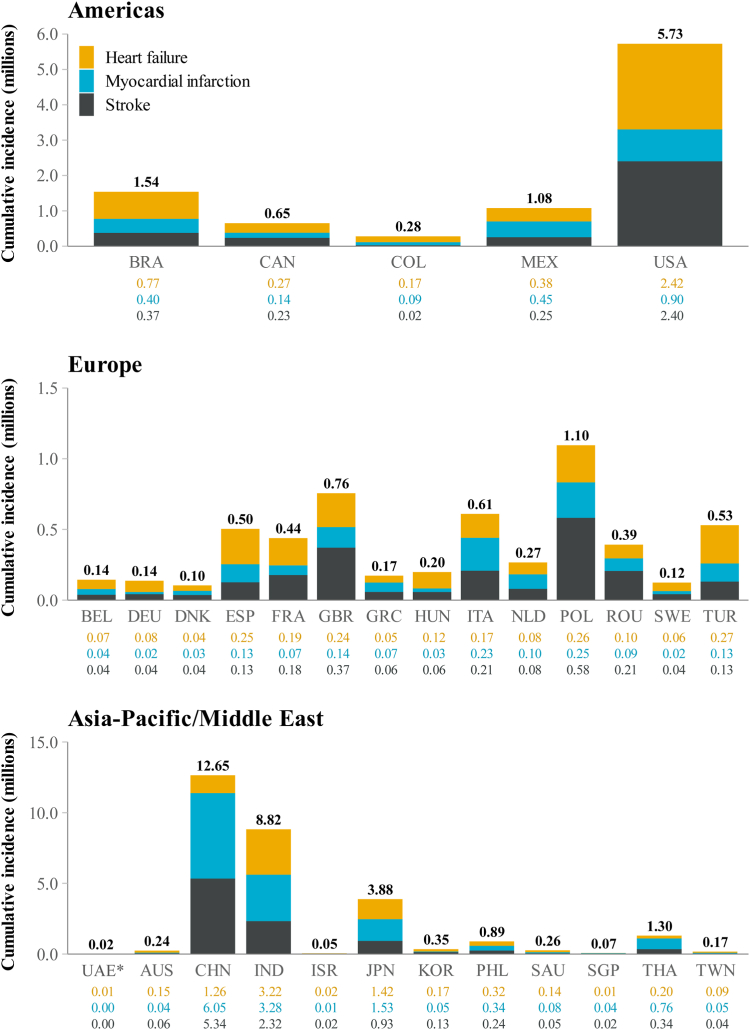
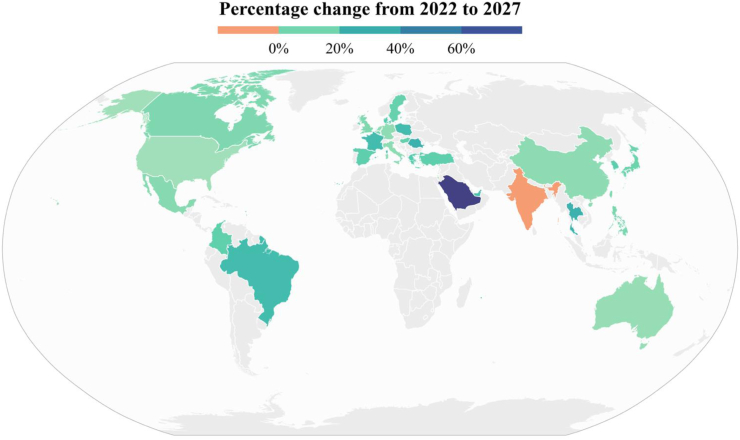
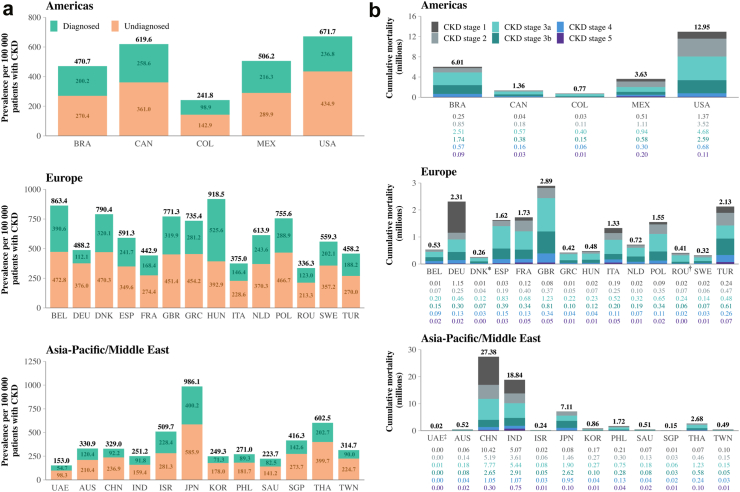
Findings: Across the 31 participating countries/regions, the total prevalence of CKD was projected to rise to 436.6 million cases by 2027 (an increase of 5.8% from 2022), with most cases (∼80%) undiagnosed. Inside CKD projected a mean of 8859 cases of heart failure, 10,244 of myocardial infarction, and 7797 of stroke per 100,000 patients with CKD by 2027.
Interpretation: The clinical impact of CKD is substantial and likely to increase; the high prevalence of undiagnosed cases and associated complications may benefit from the implementation of health policy interventions that promote screening, earlier diagnosis, and interventions to improve outcomes.
Funding: AstraZeneca.
Keywords: Burden of disease; Chronic kidney disease; Epidemiology; Microsimulation; Policy.
© 2024 The Author(s).
Conflict of interest statement
AK has received honoraria for lectures from AstraZeneca. ECH, GL, EK, CFC and RCR have received support from AstraZeneca for their contributions to this work. Stanford University School of Medicine has received grants/contracts from NIDDK, NIAID and CSL Behring on behalf of work conducted by GMC. GMC has received consulting fees from AstraZeneca, Akebia, Ardelyx, Renibus, Miromatrix, Sanifit, Unicycive and Vertex. GMC has received royalties/licences from Elsevier. GMC has participated in advisory boards/data safety monitoring boards by Bayer, Mineralys and ReCor. GMC has a leadership/fiduciary role with Satellite Healthcare Board of Directors (which is non-profit). GMC has stock/stock options at Applaud, CloudCath, Durect, Eliaz Therapeutics, Miromatrix, Outset, Renibus and Unicycive. K-UE has received grants from AstraZeneca, Amgen, Bayer, Evotec and Vifor. K-UE has received consulting fees from Akebia, AstraZeneca, Bayer, Otsuka and Retrophin. K-UE has received honoraria/payment for lectures by AstraZeneca and Bayer. K-UE has participated in advisory boards/data safety monitoring boards by AstraZeneca. LR, LW and TC are employees of HealthLumen Ltd, and AstraZeneca provided funding to HealthLumen Ltd for their contributions to this work. HealThink received funding from AstraZeneca based on the contributions of PS to this work. RCR has received grants/contracts from AstraZeneca. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán has received grants/contracts from Boehringer Ingelheim, Novo Nordisk, Roche and Baxter on behalf of work conducted by RCR. RCR has received consulting feeds from Chinook, Boehringer, Bayer and Medxl. RCR has received honoraria/payment for lectures by AstraZeneca, Amgen, Boehringer, Novo Nordisk and Bayer. SEHA Kidney Care received honoraria payments from AstraZeneca for the contributions of SGH to this work. JJGS, SB, CC and SN are employees and shareholders of AstraZeneca.
Figures
References
-
- Lamb E.J., Levey A.S., Stevens P.E. The kidney disease improving global outcomes (KDIGO) guideline update for chronic kidney disease: evolution not revolution. Clin Chem. 2013;59(3):462–465. - PubMed
-
- Chang A., Kramer H. CKD progression: a risky business. Nephrol Dial Transplant. 2012;27(7):2607–2609. - PubMed
LinkOut - more resources
Full Text Sources
