

This is a preprint.
Molecular Phenotyping of Patients with Sepsis and Kidney Injury and Differential Response to Fluid Resuscitation
- PMID: 39011119
- PMCID: PMC11247924
- DOI: 10.21203/rs.3.rs-4523416/v1
Molecular Phenotyping of Patients with Sepsis and Kidney Injury and Differential Response to Fluid Resuscitation
Update in
-
Molecular Phenotyping of Sepsis and Differential Response to Fluid Resuscitation.Am J Respir Crit Care Med. 2025 Sep;211(9):1681-1688. doi: 10.1164/rccm.202412-2377OC. Am J Respir Crit Care Med. 2025. PMID: 40668865 Clinical Trial.
Abstract
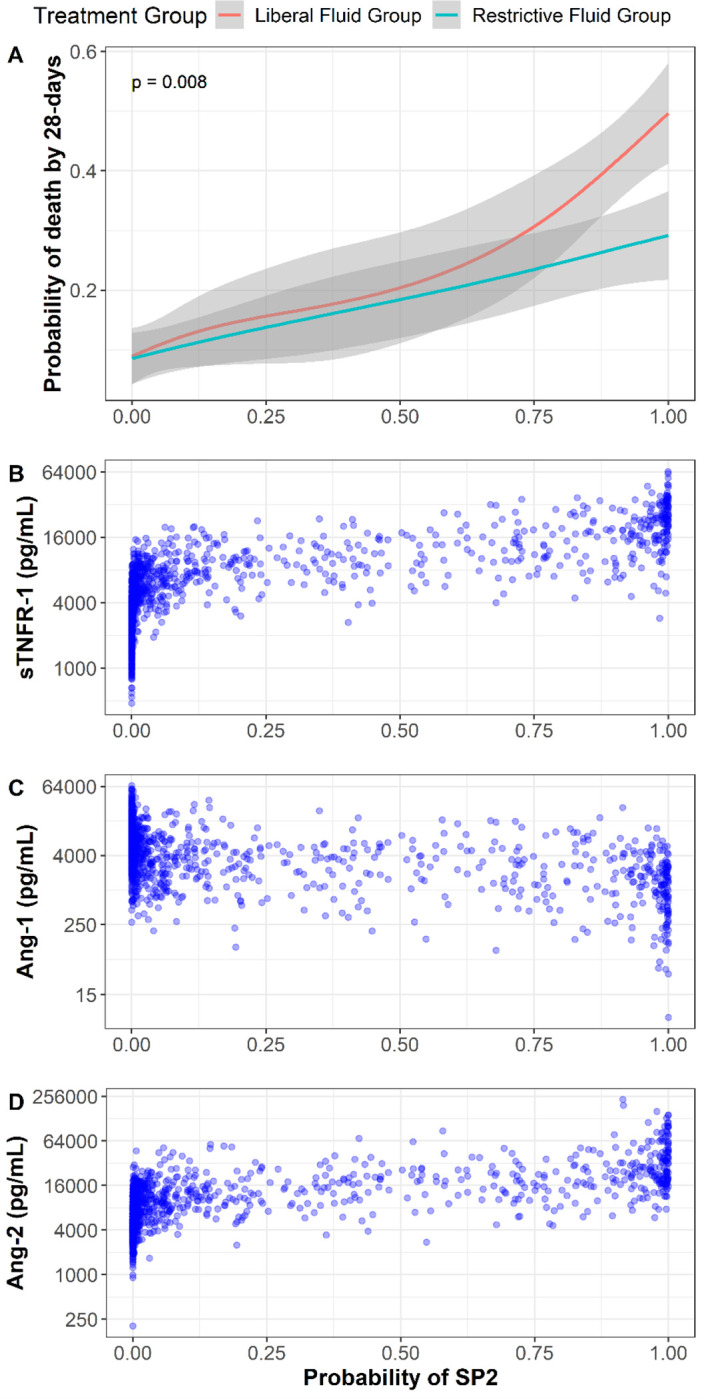
Purpose: Previous work has identified two AKI sub-phenotypes (SP1 and SP2) characterized by differences in inflammation and endothelial dysfunction. Here we identify these sub-phenotypes using biospecimens collected in the emergency department and test for differential response to restrictive versus liberal fluid strategy in sepsis-induced hypotension in the CLOVERS trial.
Methods: We applied a previously validated 3-biomarker model using plasma angiopietin-1 and 2, and soluble tumor necrosis factor receptor-1 to classify sub-phenotypes in patients with kidney dysfunction (AKI or end-stage kidney disease [ESKD]). We also compared a de novo latent class analysis (LCA) to the 3-biomarker based sub-phenotypes. Kaplan-Meier estimates were used to test for differences in outcomes and sub-phenotype by treatment interaction.
Results: Among 1289 patients, 846 had kidney dysfunction on enrollment and the 3-variable prediction model identified 605 as SP1 and 241 as SP2. The optimal LCA model identified two sub-phenotypes with high correlation with the 3-biomarker model (Cohen's Kappa 0.8). The risk of 28 and 90-day mortality was greater in SP2 relative to SP1 independent of AKI stage and SOFA scores. Patients with SP2, characterized by more severe endothelial injury and inflammation, had a reduction in 28-day mortality with a restrictive fluid strategy versus a liberal fluid strategy (26% vs 41%), while patients with SP1 had no difference in 28-day mortality (10% vs 11%) (p-value-for-interaction = 0.03).
Conclusion: Sub-phenotypes can be identified in the emergency department that respond differently to fluid strategy in sepsis. Identification of these sub-phenotypes could inform a precision-guided therapeutic approach for patients with sepsis-induced hypotension and kidney injury.
Keywords: acute kidney injury; sepsis; vasopressors; volume.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
