

Pyrazinamide Safety, Efficacy, and Dosing for Treating Drug-Susceptible Pulmonary Tuberculosis: A Phase 3, Randomized Controlled Clinical Trial
- PMID: 39012226
- PMCID: PMC11622436
- DOI: 10.1164/rccm.202401-0165OC
Pyrazinamide Safety, Efficacy, and Dosing for Treating Drug-Susceptible Pulmonary Tuberculosis: A Phase 3, Randomized Controlled Clinical Trial
Abstract
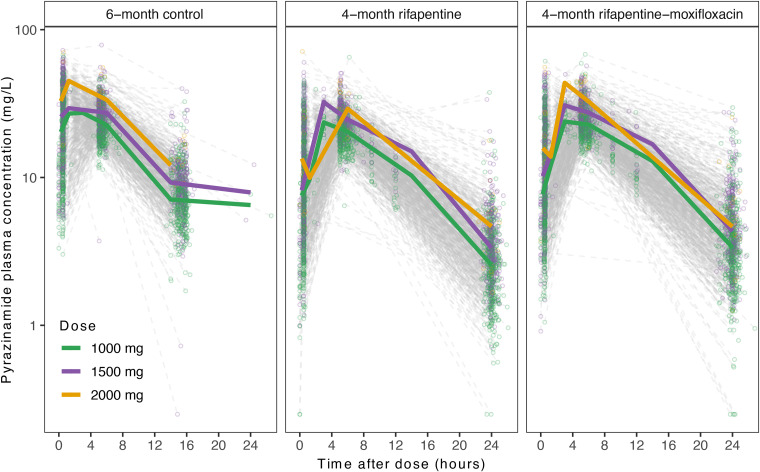
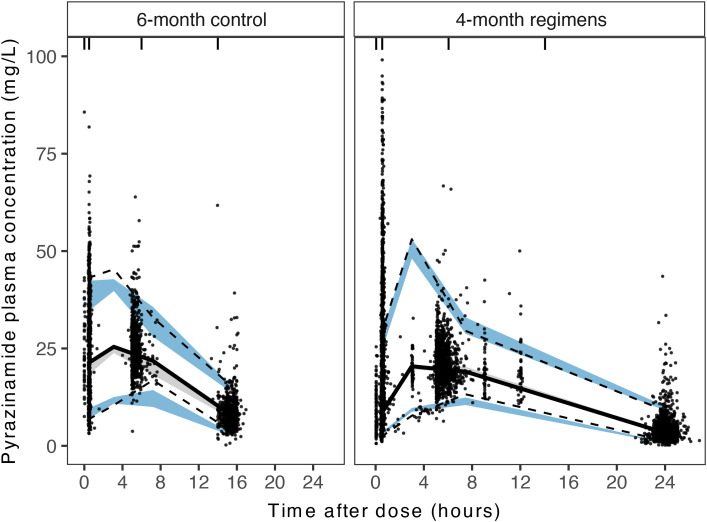
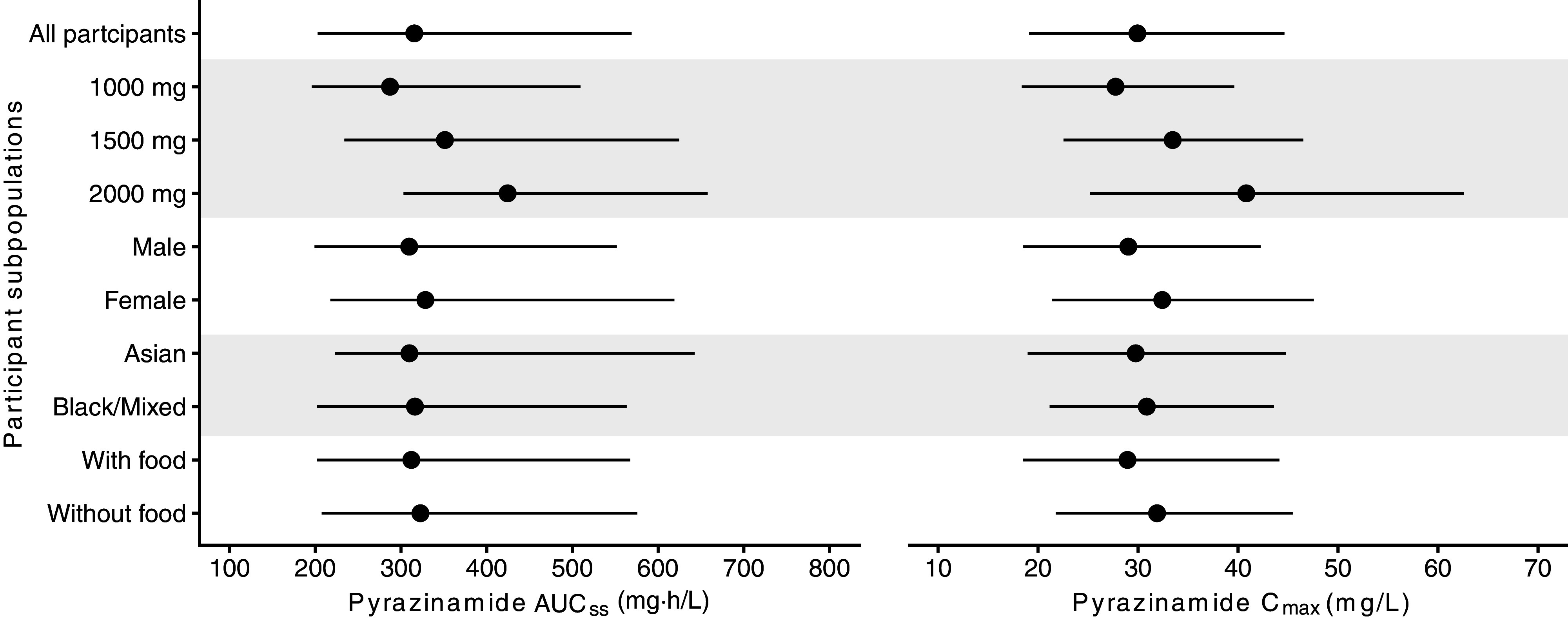
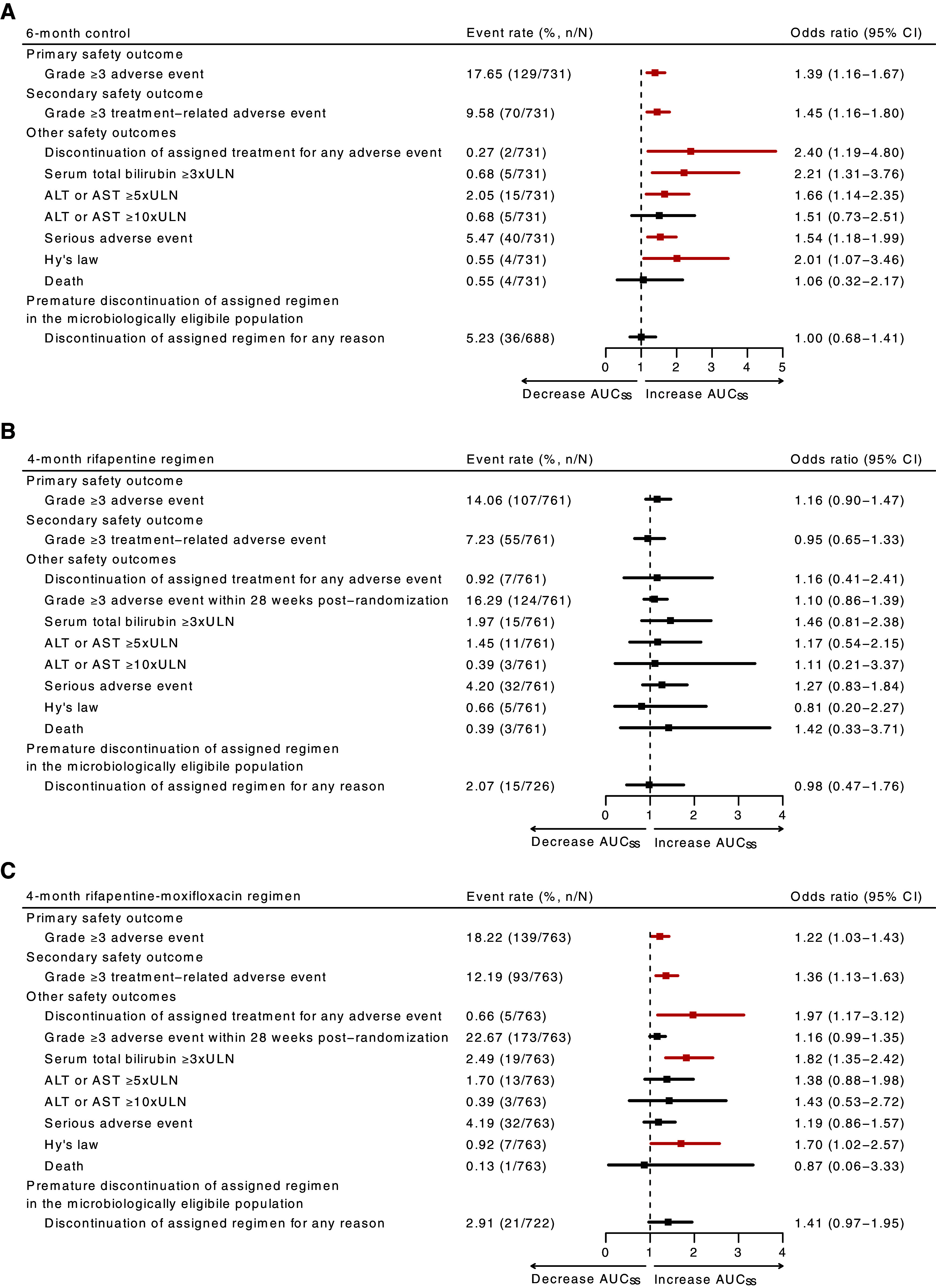
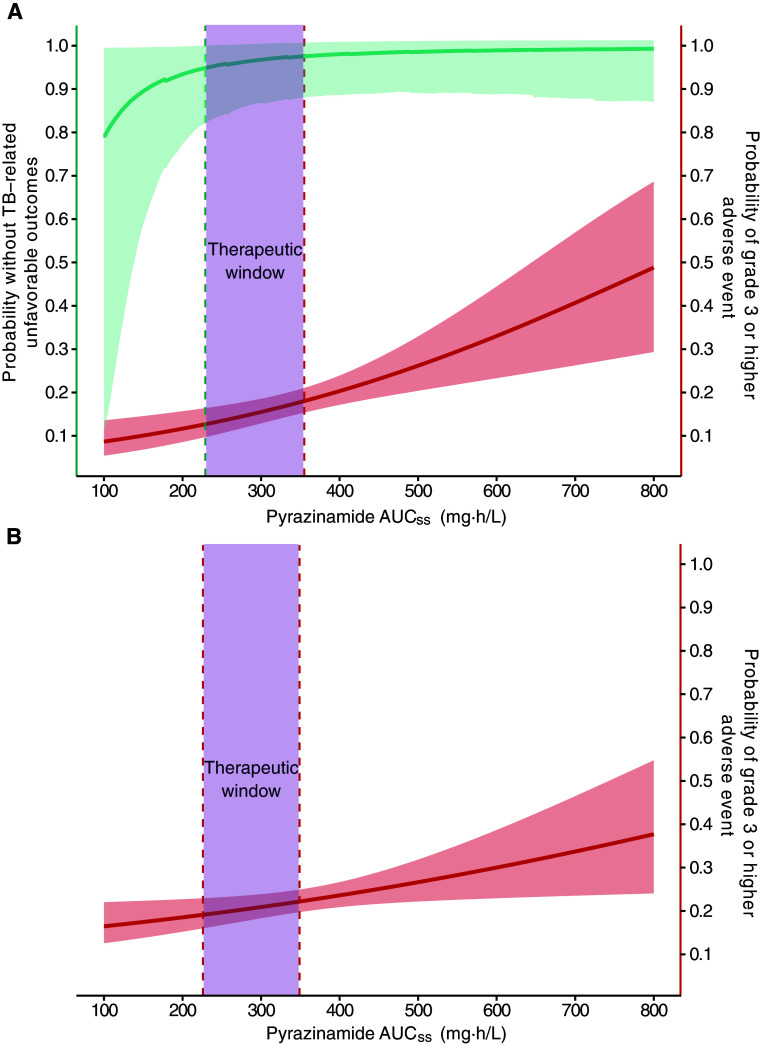
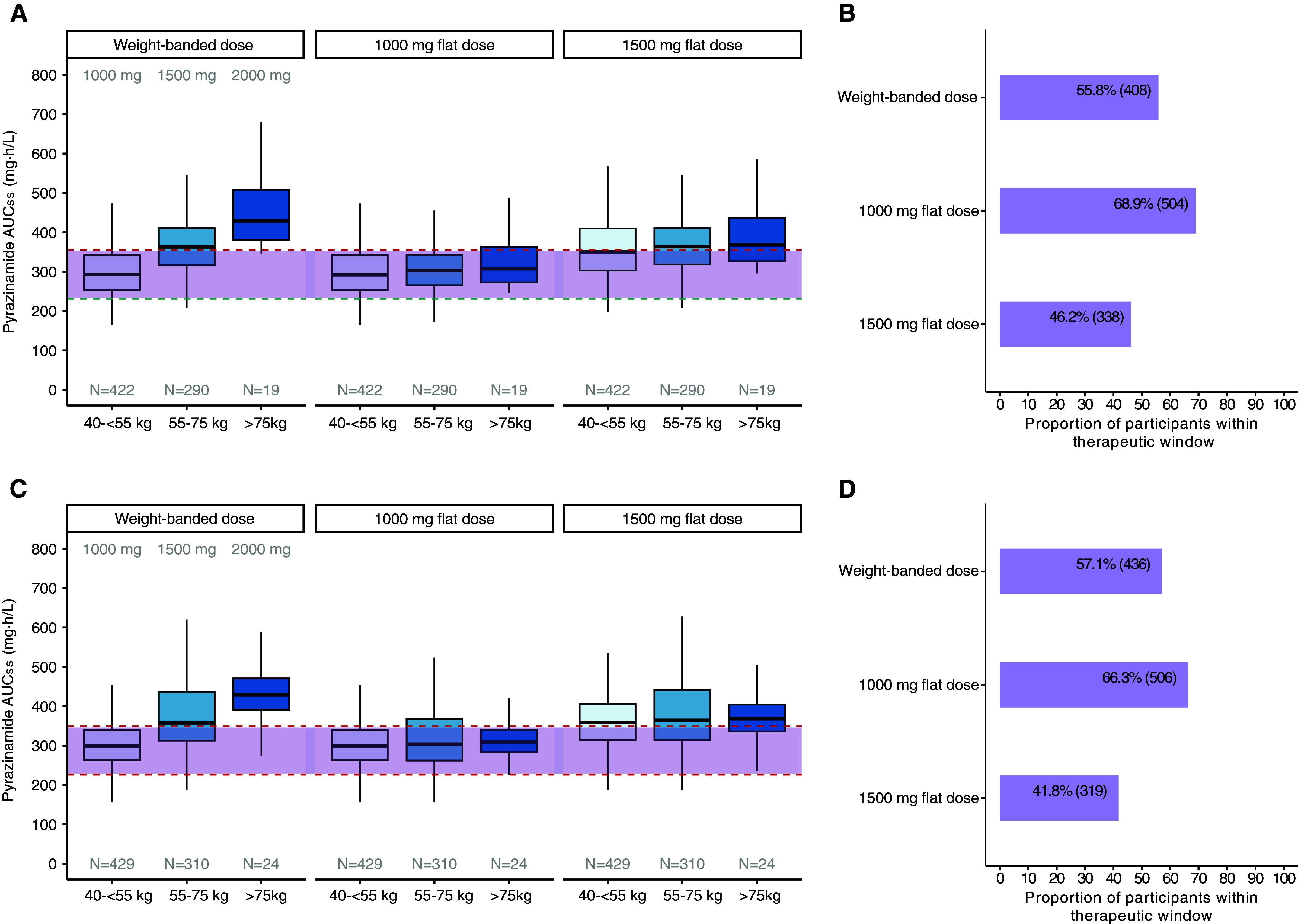
Rationale: Optimizing pyrazinamide dosing is critical to improve treatment efficacy while minimizing toxicity during tuberculosis treatment. Study 31/AIDS Clinical Trials Group A5349 represents the largest phase 3 randomized controlled therapeutic trial to date for such an investigation. Objectives: We sought to report pyrazinamide pharmacokinetic parameters, risk factors for lower pyrazinamide exposure, and relationships between pyrazinamide exposure and efficacy and safety outcomes. We aimed to determine pyrazinamide dosing strategies that optimize risks and benefits. Methods: We analyzed pyrazinamide steady-state pharmacokinetic data using population nonlinear mixed-effects models. We evaluated the contribution of pyrazinamide exposure to long-term efficacy using parametric time-to-event models and safety outcomes using logistic regression. We evaluated optimal dosing with therapeutic windows targeting ≥95% durable cure and safety within the observed proportion of the primary safety outcome. Measurements and Main Results: Among 2,255 participants with 6,978 plasma samples, pyrazinamide displayed sevenfold exposure variability (151-1,053 mg·h/L). Body weight was not a clinically relevant predictor of drug clearance and thus did not justify the need for weight-banded dosing. Both clinical and safety outcomes were associated with pyrazinamide exposure, resulting in therapeutic windows of 231-355 mg · h/L for the control and 226-349 mg·h/L for the rifapentine-moxifloxacin regimen. Flat dosing of pyrazinamide at 1,000 mg would have permitted an additional 13.1% (n = 96) of participants allocated to the control and 9.2% (n = 70) to the rifapentine-moxifloxacin regimen dosed within the therapeutic window, compared with the current weight-banded dosing. Conclusions: Flat dosing of pyrazinamide at 1,000 mg/d would be readily implementable and could optimize treatment outcomes in drug-susceptible tuberculosis. Clinical trial registered with www.clinicaltrials.gov (NCT02410772).
Keywords: dose–response; exposure–response; population pharmacokinetics; pyrazinamide; tuberculosis.
Figures
Comment in
-
A Balancing Act: Finding the Right Dose of Pyrazinamide to Treat Tuberculosis.Am J Respir Crit Care Med. 2024 Dec 1;210(11):1295-1296. doi: 10.1164/rccm.202406-1262ED. Am J Respir Crit Care Med. 2024. PMID: 39173151 Free PMC article. No abstract available.
References
-
- World Health Organization. Global tuberculosis report 2023. Geneva, Switzerland: World Health Organization; 2023.
-
- Hu Y, Coates AR, Mitchison DA. Sterilising action of pyrazinamide in models of dormant and rifampicin-tolerant Mycobacterium tuberculosis. Int J Tuberc Lung Dis . 2006;10:317–322. - PubMed
-
- Phillips S, Larkin JC, Jr, Litzenberger WL, Horton GE, Haimsohn JS. Observations on pyrazinamide (Aldinamide) in pulmonary tuberculosis. Am Rev Tuberc . 1954;69:443–450. - PubMed
