

Identification and validation of a machine learning model of complete response to radiation in rectal cancer reveals immune infiltrate and TGFβ as key predictors
- PMID: 39013324
- PMCID: PMC11663784
- DOI: 10.1016/j.ebiom.2024.105228
Identification and validation of a machine learning model of complete response to radiation in rectal cancer reveals immune infiltrate and TGFβ as key predictors
Abstract
Background: It is uncertain which biological features underpin the response of rectal cancer (RC) to radiotherapy. No biomarker is currently in clinical use to select patients for treatment modifications.
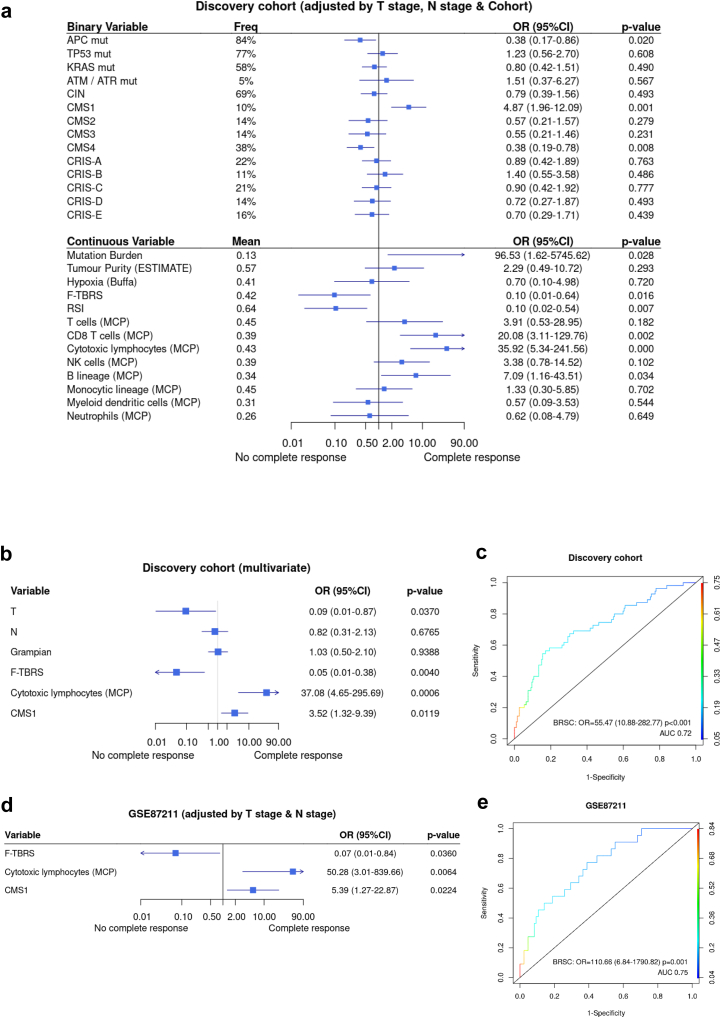
Methods: We identified two cohorts of patients (total N = 249) with RC treated with neoadjuvant radiotherapy (45Gy/25) plus fluoropyrimidine. This discovery set included 57 cases with pathological complete response (pCR) to chemoradiotherapy (23%). Pre-treatment cancer biopsies were assessed using transcriptome-wide mRNA expression and targeted DNA sequencing for copy number and driver mutations. Biological candidate and machine learning (ML) approaches were used to identify predictors of pCR to radiotherapy independent of tumour stage. Findings were assessed in 107 cases from an independent validation set (GSE87211).
Findings: Three gene expression sets showed significant independent associations with pCR: Fibroblast-TGFβ Response Signature (F-TBRS) with radioresistance; and cytotoxic lymphocyte (CL) expression signature and consensus molecular subtype CMS1 with radiosensitivity. These associations were replicated in the validation cohort. In parallel, a gradient boosting machine model comprising the expression of 33 genes generated in the discovery cohort showed high performance in GSE87211 with 90% sensitivity, 86% specificity. Biological and ML signatures indicated similar mechanisms underlying radiation response, and showed better AUC and p-values than published transcriptomic signatures of radiation response in RC.
Interpretation: RCs responding completely to chemoradiotherapy (CRT) have biological characteristics of immune response and absence of immune inhibitory TGFβ signalling. These tumours may be identified with a potential biomarker based on a 33 gene expression signature. This could help select patients likely to respond to treatment with a primary radiotherapy approach as for anal cancer. Conversely, those with predicted radioresistance may be candidates for clinical trials evaluating addition of immune-oncology agents and stromal TGFβ signalling inhibition.
Funding: The Stratification in Colorectal Cancer Consortium (S:CORT) was funded by the Medical Research Council and Cancer Research UK (MR/M016587/1).
Keywords: Genes; Immune response; Precision medicine; Prediction; Radiotherapy; Rectal neoplasms; TGFβ.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests TSM is now employed by the University of Liverpool and acknowledges consultancy payments from Astrazeneca, Ground Truth Laboratories and Nordic Pharma. V.H.K. has served as an invited speaker on behalf of Indica Labs. U.M is now employed by and holds stocks in Astrazeneca. Other authors declare no conflict of interests.
Figures





References
-
- Chemotherapy, radiotherapy and tumour resections in England: 2013-2021. https://digital.nhs.uk/data-and-information/publications/statistical/che...
-
- Benson A.B., Venook A.P., Al-Hawary M.M., et al. NCCN guidelines insights: rectal cancer, version 6.2020. J Natl Compr Canc Netw. 2020;18(7):806–815. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
