

Immunomic longitudinal profiling of the NeoPembrOv trial identifies drivers of immunoresistance in high-grade ovarian carcinoma
- PMID: 39013886
- PMCID: PMC11252308
- DOI: 10.1038/s41467-024-47000-5
Immunomic longitudinal profiling of the NeoPembrOv trial identifies drivers of immunoresistance in high-grade ovarian carcinoma
Abstract
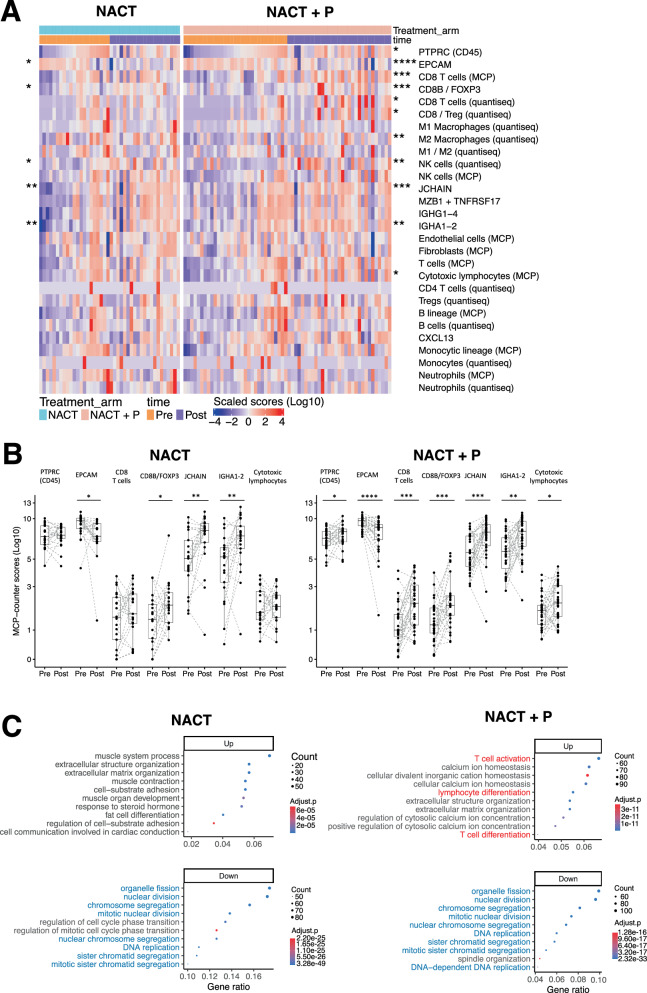
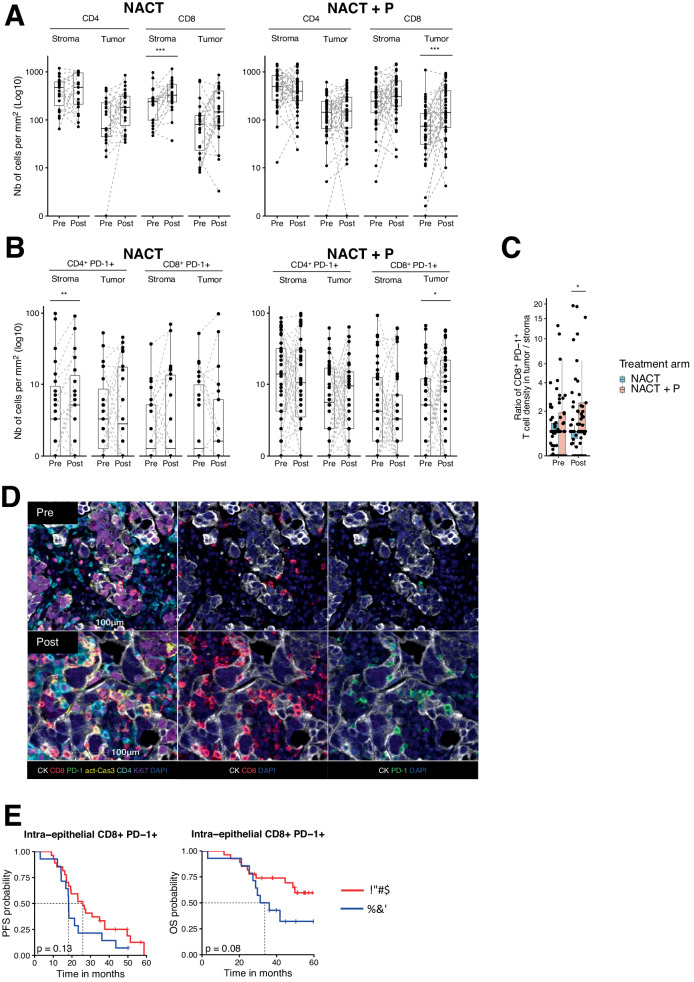
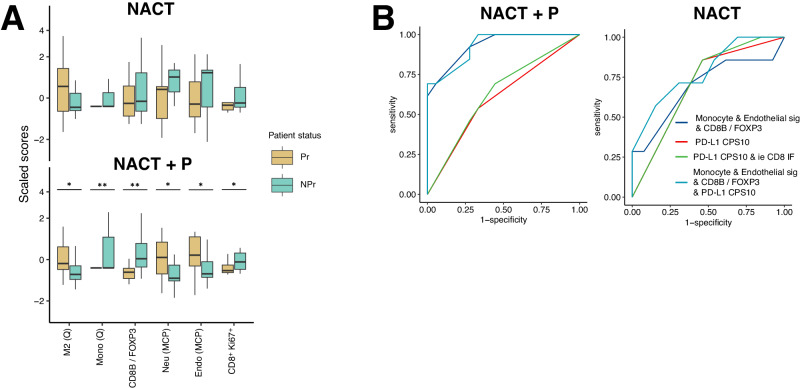
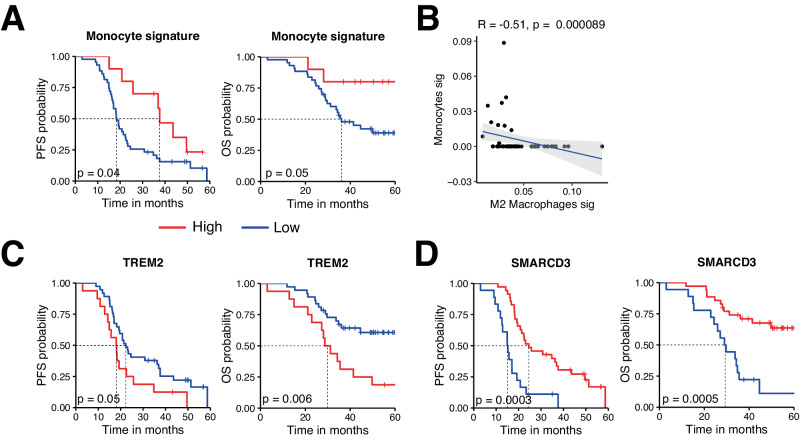
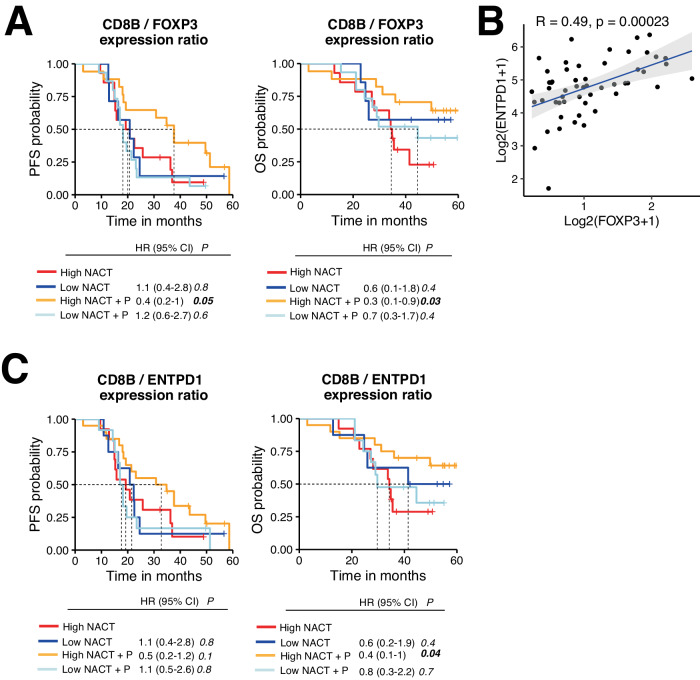
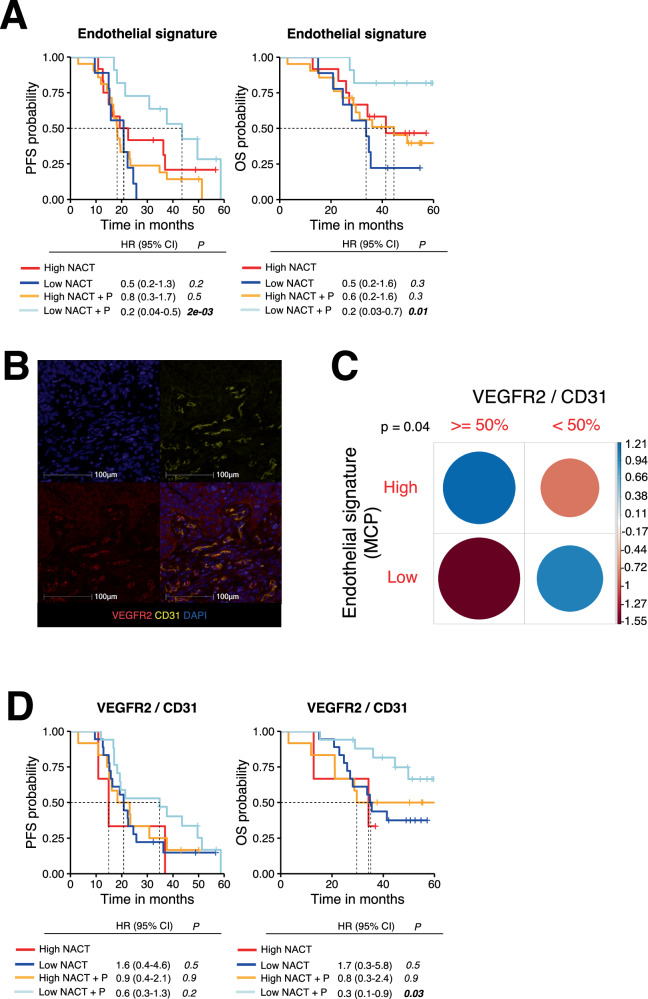
PD-1/PD-L1 blockade has so far shown limited survival benefit for high-grade ovarian carcinomas. By using paired samples from the NeoPembrOv randomized phase II trial (NCT03275506), for which primary outcomes are published, and by combining RNA-seq and multiplexed immunofluorescence staining, we explore the impact of NeoAdjuvant ChemoTherapy (NACT) ± Pembrolizumab (P) on the tumor environment, and identify parameters that correlated with response to immunotherapy as a pre-planned exploratory analysis. Indeed, i) combination therapy results in a significant increase in intraepithelial CD8+PD-1+ T cells, ii) combining endothelial and monocyte gene signatures with the CD8B/FOXP3 expression ratio is predictive of response to NACT + P with an area under the curve of 0.93 (95% CI 0.85-1.00) and iii) high CD8B/FOXP3 and high CD8B/ENTPD1 ratios are significantly associated with positive response to NACT + P, while KDR and VEGFR2 expression are associated with resistance. These results indicate that targeting regulatory T cells and endothelial cells, especially VEGFR2+ endothelial cells, could overcome immune resistance of ovarian cancers.
© 2024. The Author(s).
Conflict of interest statement
O.L.S. reports honoraria from MSD and Clovis, and travel/accommodation/expenses from Eisai. E.C. reports the following, all for an immediate family member: employment with Sanofi; consulting/advisory role for MSD, BMS, Ipsen, and AstraZeneca; speakers’ bureau for BMS, Ipsen, AstraZeneca, and Janssen; research funding from Pfizer; and travel/accommodation/expenses from Janssen. I.R-C reports personal honoraria from Agenus, Blueprint, BMS, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche, GSK, MSD, Deciphera, Mersana, Merck Sereno, Novartis, Amgen, MacroGenics, Tesaro, and Clovis; honoraria to her institution from GSK, MSD, Roche, and BMS; consulting/advisory roles for AbbVie, Agenus, Advaxis, BMS, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche/Genentech, GSK, MSD, Deciphera, Mersana, Merck Sereno, Novartis, Amgen, Tesaro and Clovis; research grant/funding from MSD, Roche and BMS (self) and MSD, Roche, BMS, Novartis, AstraZeneca and Merck Sereno (to institution); and travel support from Roche, AstraZeneca, and GSK. Other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
