

At-admission prediction of mortality and pulmonary embolism in an international cohort of hospitalised patients with COVID-19 using statistical and machine learning methods
- PMID: 39013928
- PMCID: PMC11252333
- DOI: 10.1038/s41598-024-63212-7
At-admission prediction of mortality and pulmonary embolism in an international cohort of hospitalised patients with COVID-19 using statistical and machine learning methods
Abstract
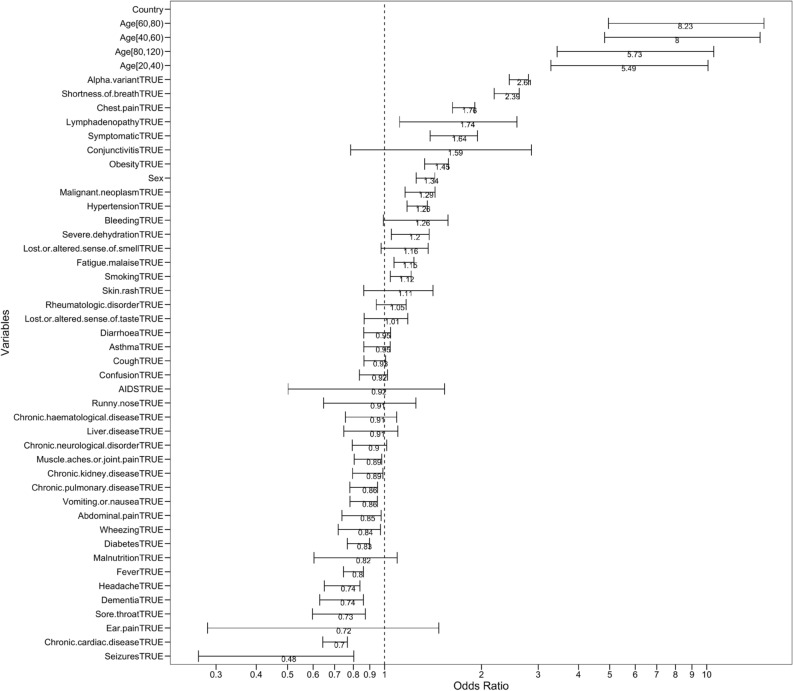
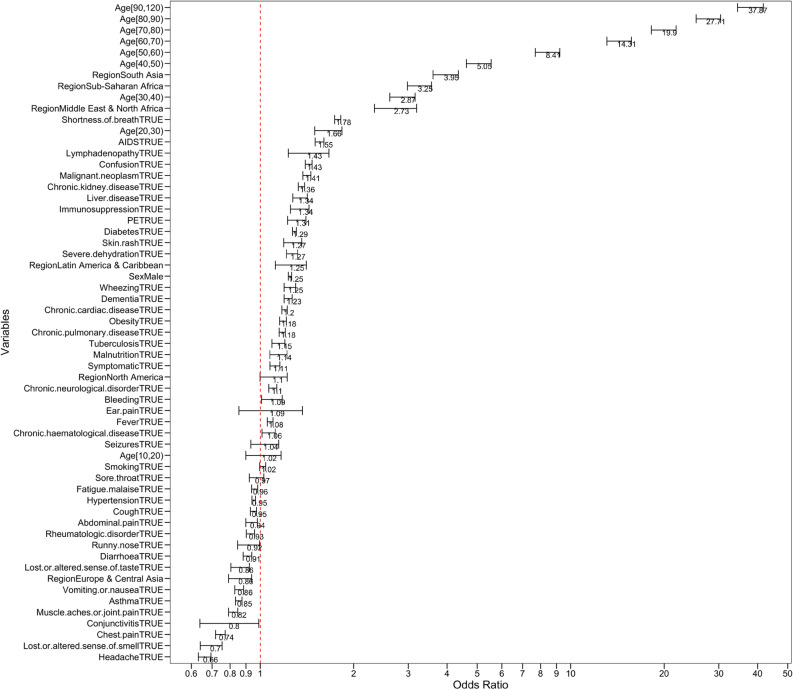
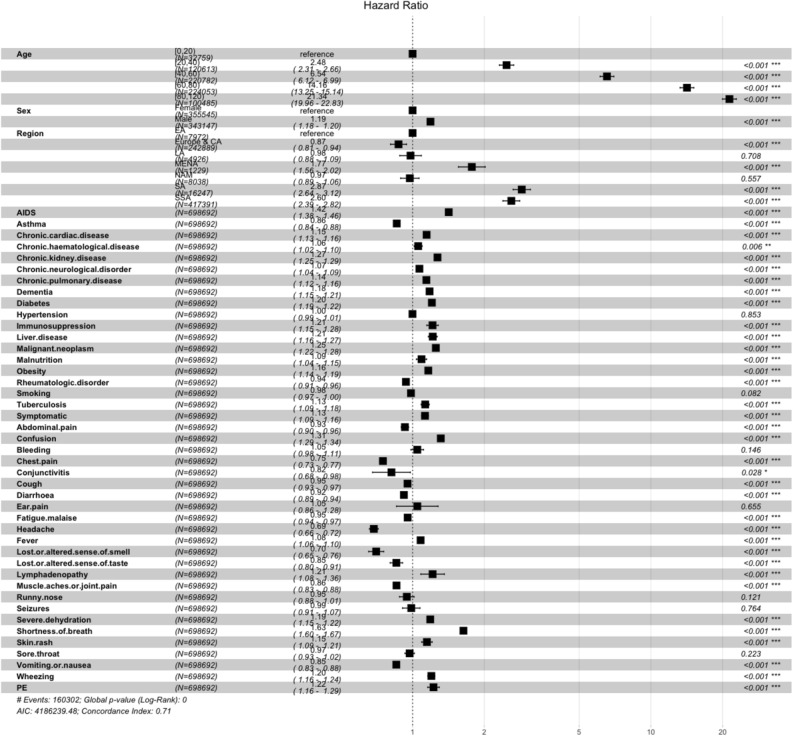
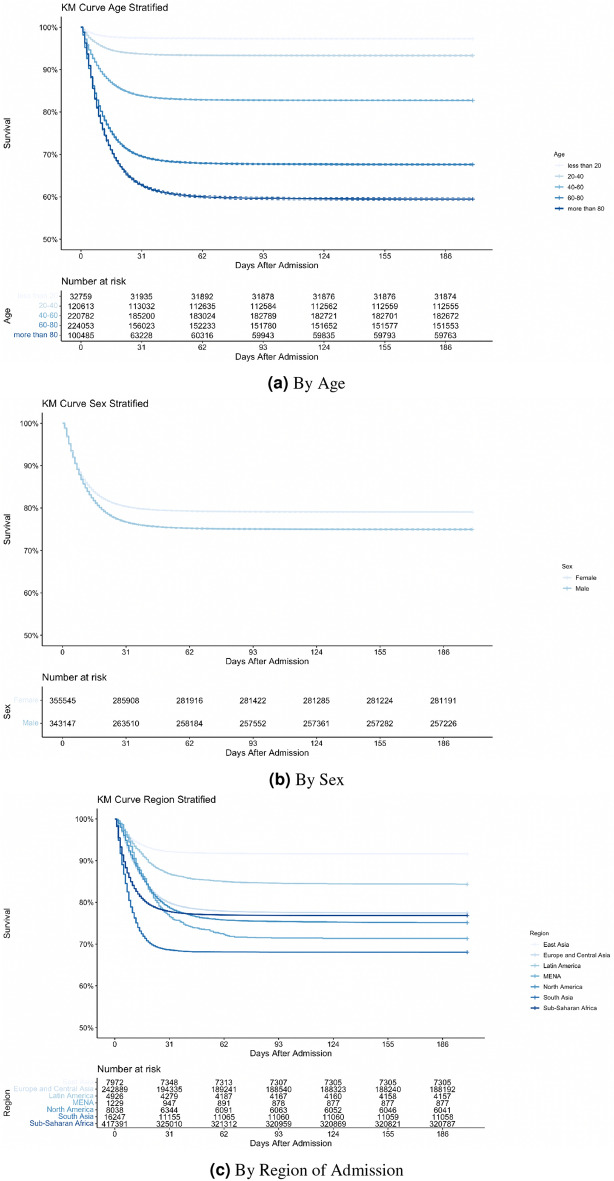
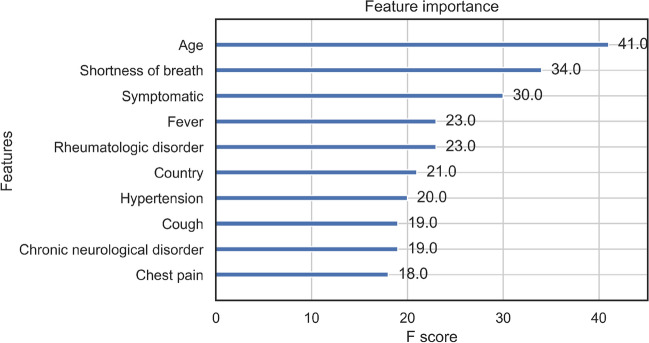
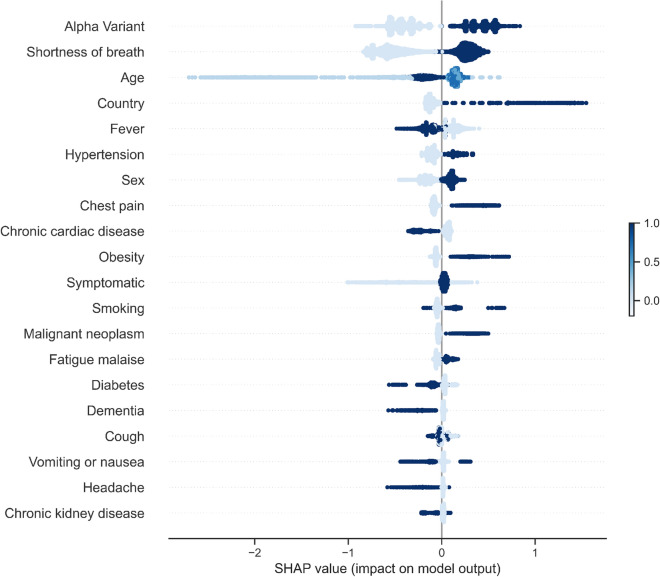
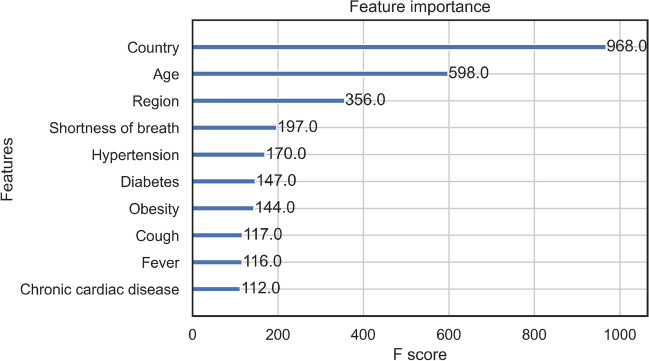
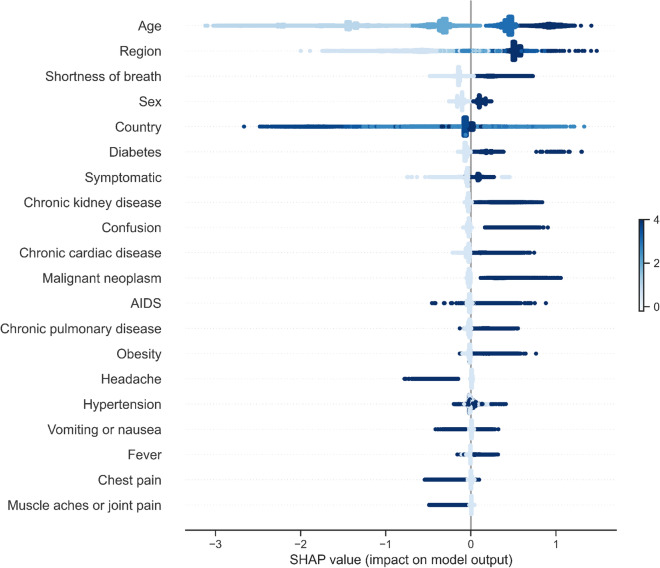
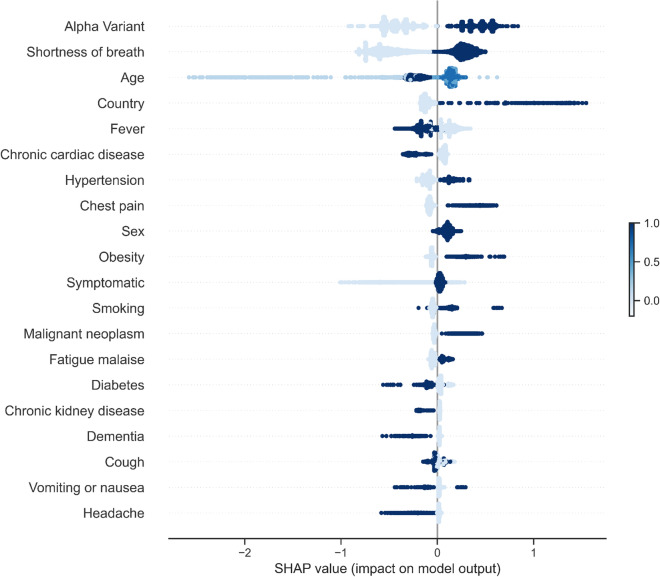
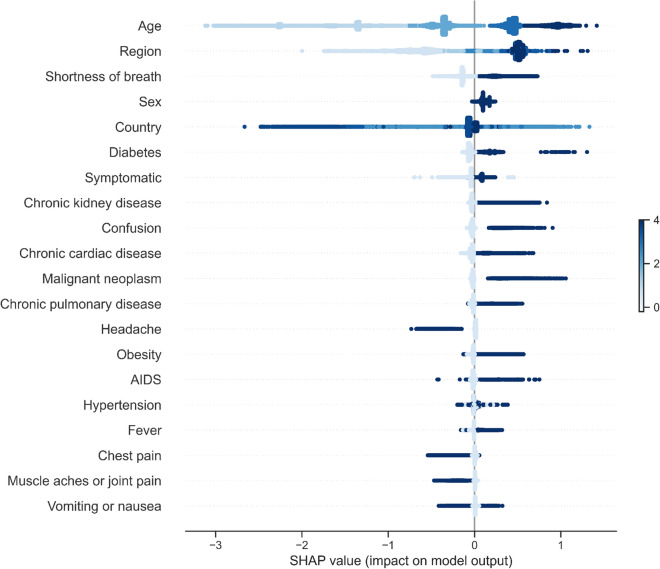
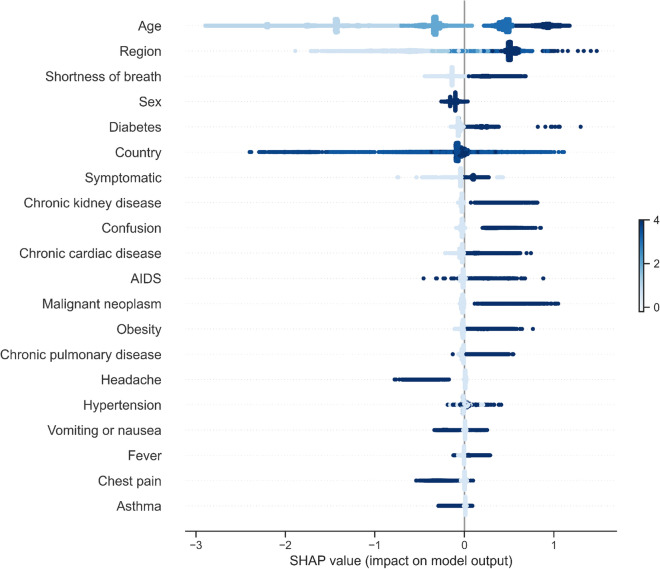
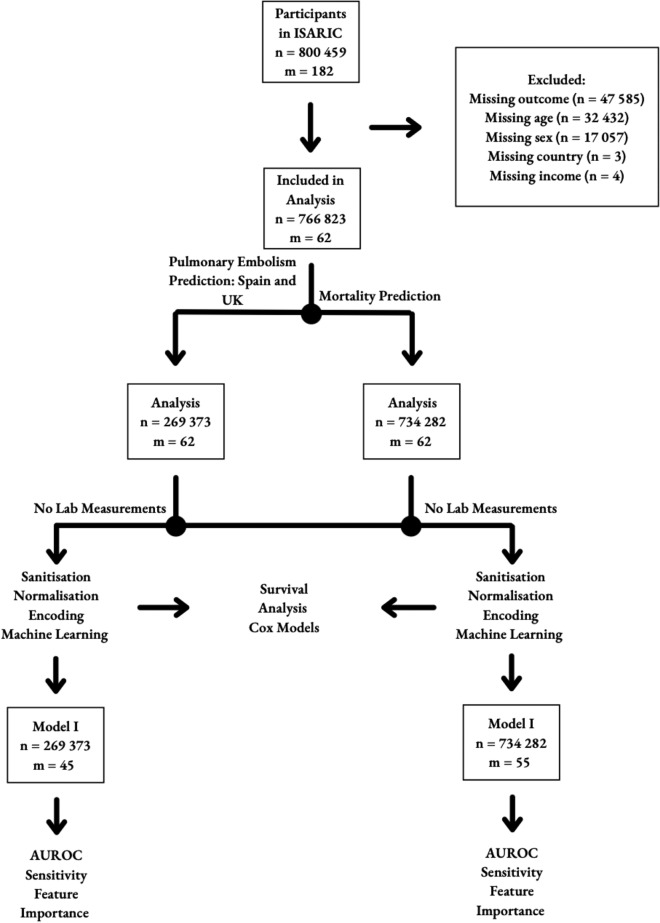
By September 2022, more than 600 million cases of SARS-CoV-2 infection have been reported globally, resulting in over 6.5 million deaths. COVID-19 mortality risk estimators are often, however, developed with small unrepresentative samples and with methodological limitations. It is highly important to develop predictive tools for pulmonary embolism (PE) in COVID-19 patients as one of the most severe preventable complications of COVID-19. Early recognition can help provide life-saving targeted anti-coagulation therapy right at admission. Using a dataset of more than 800,000 COVID-19 patients from an international cohort, we propose a cost-sensitive gradient-boosted machine learning model that predicts occurrence of PE and death at admission. Logistic regression, Cox proportional hazards models, and Shapley values were used to identify key predictors for PE and death. Our prediction model had a test AUROC of 75.9% and 74.2%, and sensitivities of 67.5% and 72.7% for PE and all-cause mortality respectively on a highly diverse and held-out test set. The PE prediction model was also evaluated on patients in UK and Spain separately with test results of 74.5% AUROC, 63.5% sensitivity and 78.9% AUROC, 95.7% sensitivity. Age, sex, region of admission, comorbidities (chronic cardiac and pulmonary disease, dementia, diabetes, hypertension, cancer, obesity, smoking), and symptoms (any, confusion, chest pain, fatigue, headache, fever, muscle or joint pain, shortness of breath) were the most important clinical predictors at admission. Age, overall presence of symptoms, shortness of breath, and hypertension were found to be key predictors for PE using our extreme gradient boosted model. This analysis based on the, until now, largest global dataset for this set of problems can inform hospital prioritisation policy and guide long term clinical research and decision-making for COVID-19 patients globally. Our machine learning model developed from an international cohort can serve to better regulate hospital risk prioritisation of at-risk patients.
© 2024. The Author(s).
Figures

References
-
- WHO. Novel coronavirus (2019-ncov): situation report, 11. (2020).
-
- University, J. H. Covid-19 dashboard by the center for systems science and engineering (csse) (2022).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
