

A randomized, embedded, pragmatic, Bayesian clinical trial examining clinical decision support for high flow nasal cannula management in children with bronchiolitis: design and statistical analysis plan
- PMID: 39014495
- PMCID: PMC11253479
- DOI: 10.1186/s13063-024-08327-y
A randomized, embedded, pragmatic, Bayesian clinical trial examining clinical decision support for high flow nasal cannula management in children with bronchiolitis: design and statistical analysis plan
Abstract
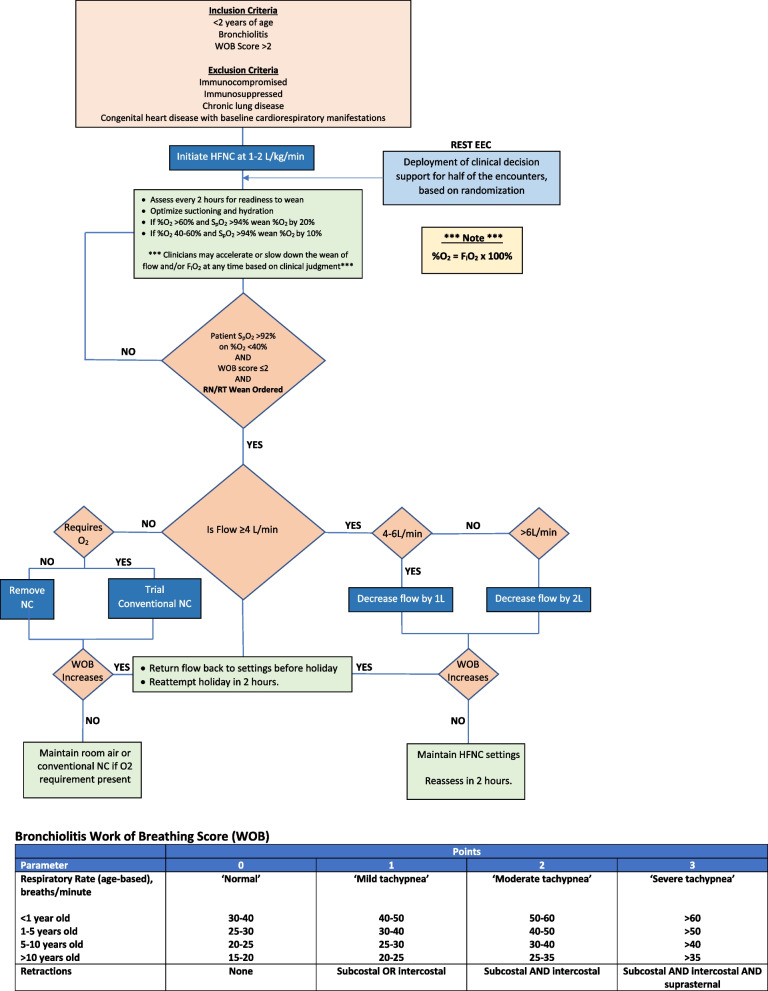
Background: High flow nasal cannula (HFNC) has been increasingly adopted in the past 2 decades as a mode of respiratory support for children hospitalized with bronchiolitis. The growing use of HFNC despite a paucity of high-quality data regarding the therapy's efficacy has led to concerns about overutilization. We developed an electronic health record (EHR) embedded, quality improvement (QI) oriented clinical trial to determine whether standardized management of HFNC weaning guided by clinical decision support (CDS) results in a reduction in the duration of HFNC compared to usual care for children with bronchiolitis.
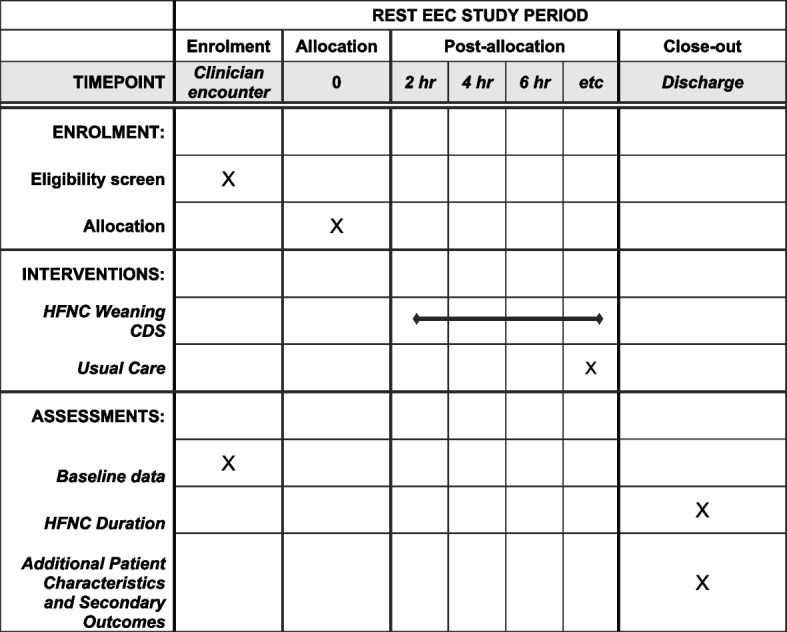
Methods: The design and summary of the statistical analysis plan for the REspiratory SupporT for Efficient and cost-Effective Care (REST EEC; "rest easy") trial are presented. The investigators hypothesize that CDS-coupled, standardized HFNC weaning will reduce the duration of HFNC, the trial's primary endpoint, for children with bronchiolitis compared to usual care. Data supporting trial design and eventual analyses are collected from the EHR and other real world data sources using existing informatics infrastructure and QI data sources. The trial workflow, including randomization and deployment of the intervention, is embedded within the EHR of a large children's hospital using existing vendor features. Trial simulations indicate that by assuming a true hazard ratio effect size of 1.27, equivalent to a 6-h reduction in the median duration of HFNC, and enrolling a maximum of 350 children, there will be a > 0.75 probability of declaring superiority (interim analysis posterior probability of intervention effect > 0.99 or final analysis posterior probability of intervention effect > 0.9) and a > 0.85 probability of declaring superiority or the CDS intervention showing promise (final analysis posterior probability of intervention effect > 0.8). Iterative plan-do-study-act cycles are used to monitor the trial and provide targeted education to the workforce.
Discussion: Through incorporation of the trial into usual care workflows, relying on QI tools and resources to support trial conduct, and relying on Bayesian inference to determine whether the intervention is superior to usual care, REST EEC is a learning health system intervention that blends health system operations with active evidence generation to optimize the use of HFNC and associated patient outcomes.
Trial registration: ClinicalTrials.gov NCT05909566. Registered on June 18, 2023.
Keywords: Bronchiolitis; Clinical informatics; Electronic health record; Pragmatic trial; Quality improvement.
© 2024. The Author(s).
Conflict of interest statement
No authors disclosed any competing interests with the design or conduct of this study.
Figures




References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
