

Young infants with symptomatic tetralogy of Fallot: Shunt or primary repair?
- PMID: 39015442
- PMCID: PMC11247207
- DOI: 10.1016/j.xjon.2024.04.003
Young infants with symptomatic tetralogy of Fallot: Shunt or primary repair?
Abstract
Objectives: The optimal treatment strategy for symptomatic young infants with tetralogy of Fallot (TOF) is unclear. We sought to compare the outcomes of staged repair (SR) (shunt palliation followed by second-stage complete repair) versus primary repair (PR) at 2 institutions that have exclusively adopted each strategy.
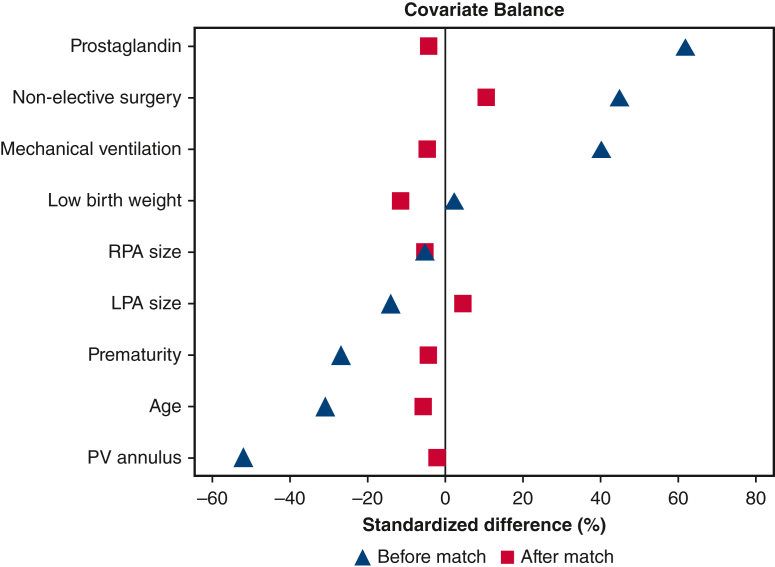
Methods: We performed propensity score-matched comparison of 143 infants under 4 months of age who underwent shunt palliation at one institution between 1993 and 2021 with 122 infants who underwent PR between 2004 and 2018 at another institution. The primary outcome was mortality. Secondary outcomes were postoperative complications, durations of perioperative support and hospital stays, and reinterventions. Median follow-up was 8.3 years (interquartile range, 8.1-13.4 years).
Results: After the initial procedure, hospital mortality (shunt, 2.8% vs PR, 2.5%; P = .86) and 10-year survival (shunt, 95%; 95% confidence interval [CI], 90%-98% vs PR, 90%; 95% CI, 81%-95%; P = .65) were similar. The SR group had a greater risk of early reinterventions but similar rates of late reinterventions. Propensity score matching yielded 57 well-balanced pairs. In the matched cohort, the SR group had similar freedom from reintervention (55%; 95% CI, 39%-68% vs 59%; 95% CI, 43%-71%; P = .85) and greater survival (98%; 95% CI, 88%-99.8% vs 85%; 95% CI, 69%-93%; P = .02) at 10 years, as the result of more noncardiac-related mortalities in the PR group.
Conclusions: In symptomatic young infants with TOF operated at 2 institutions with exclusive treatment protocols, the SR strategy was associated with similar cardiac-related mortality and reinterventions as the PR strategy at medium-term follow-up.
Keywords: infants; palliation; surgery; symptomatic; tetralogy of Fallot.
Crown Copyright © 2024 Published by Elsevier Inc. on behalf of The American Association for Thoracic Surgery.
Conflict of interest statement
Dr Brizard has served on the advisory board of Admedus. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures






References
-
- Miller J.R., Stephens E.H., Goldstone A.B., et al. The American Association for Thoracic Surgery (AATS) 2022 Expert Consensus Document: management of infants and neonates with tetralogy of Fallot. J Thorac Cardiovasc Surg. 2023;165(1):221–250. - PubMed
-
- Zurakowski D., Jonas R.A. The many factors leading to resurgence of the Blalock shunt for tetralogy. J Thorac Cardiovasc Surg. 2021;161(2):396–399. - PubMed
-
- Ramakrishnan K.V., Zurakowski D., Pastor W., Jonas R.A., Sinha P. Symptomatic tetralogy of Fallot in young infants: primary repair or shunt-Pediatric Health Information System Database analysis. World J Pediatr Congenit Heart Surg. 2018;9(5):539–545. - PubMed
-
- Steiner M.B., Tang X., Gossett J.M., et al. Alternative repair strategies for ductal-dependent tetralogy of Fallot and short-term postoperative outcomes, a multicenter analysis. Pediatr Cardiol. 2015;36(1):177–189. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
