

Loss of tolerance precedes triggering and lifelong persistence of pathogenic type I interferon autoantibodies
- PMID: 39017930
- PMCID: PMC11253716
- DOI: 10.1084/jem.20240365
Loss of tolerance precedes triggering and lifelong persistence of pathogenic type I interferon autoantibodies
Abstract
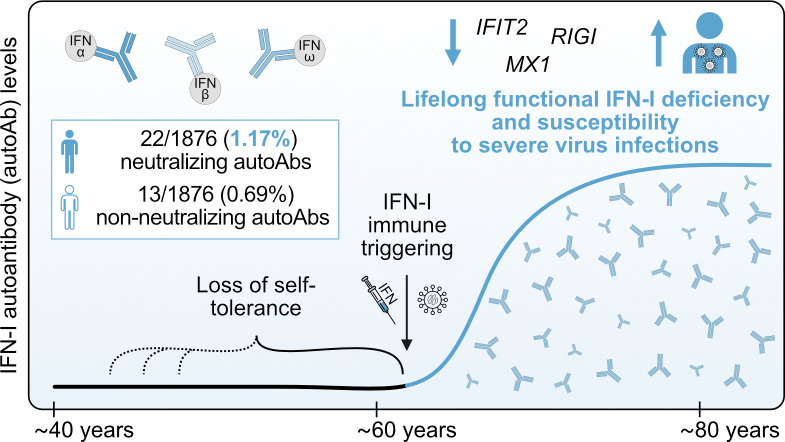
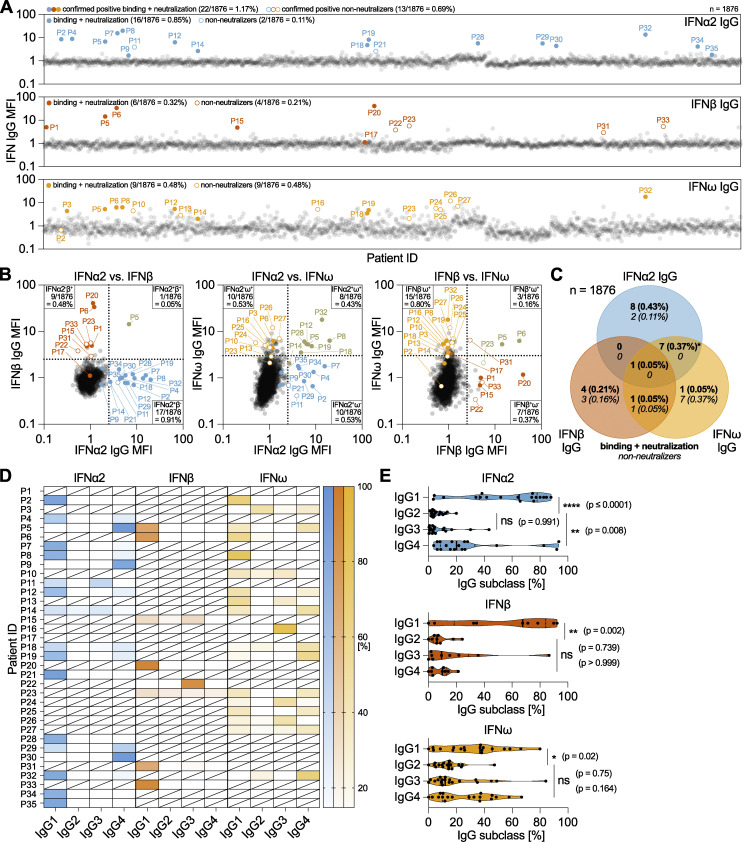
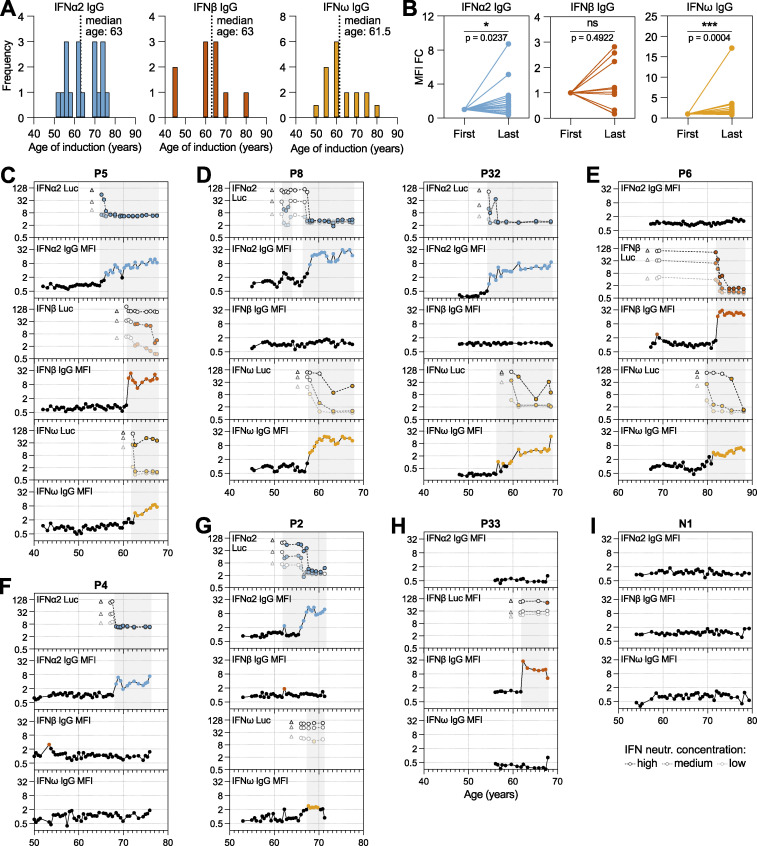
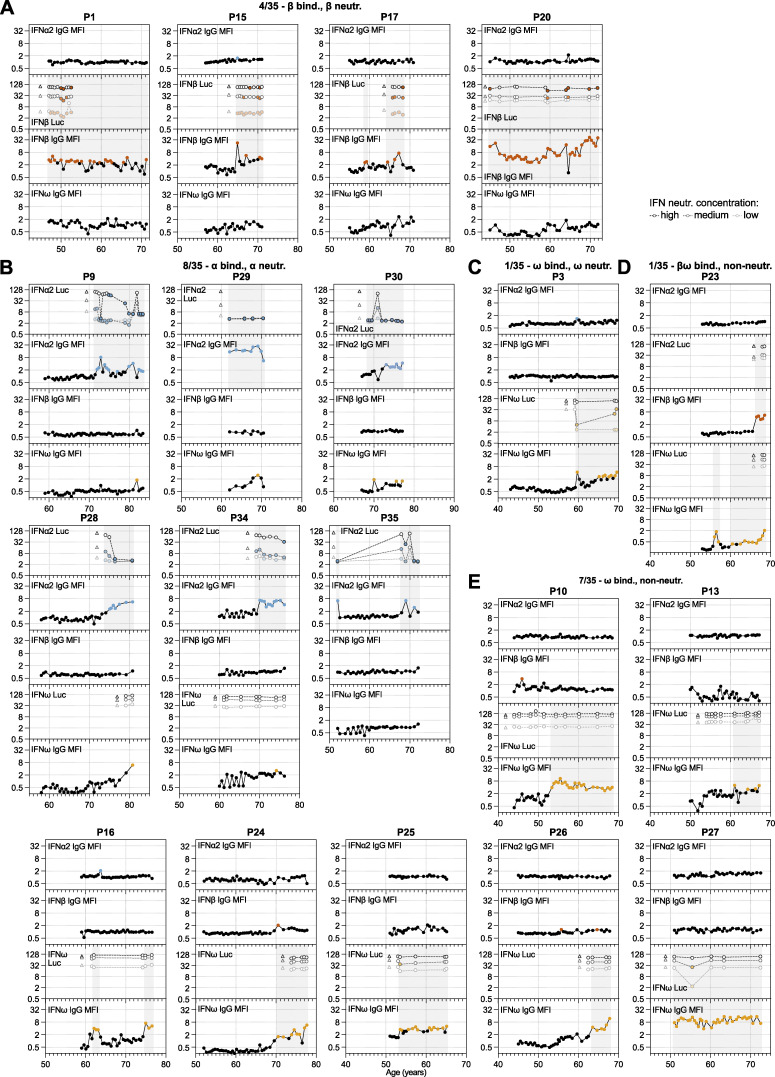
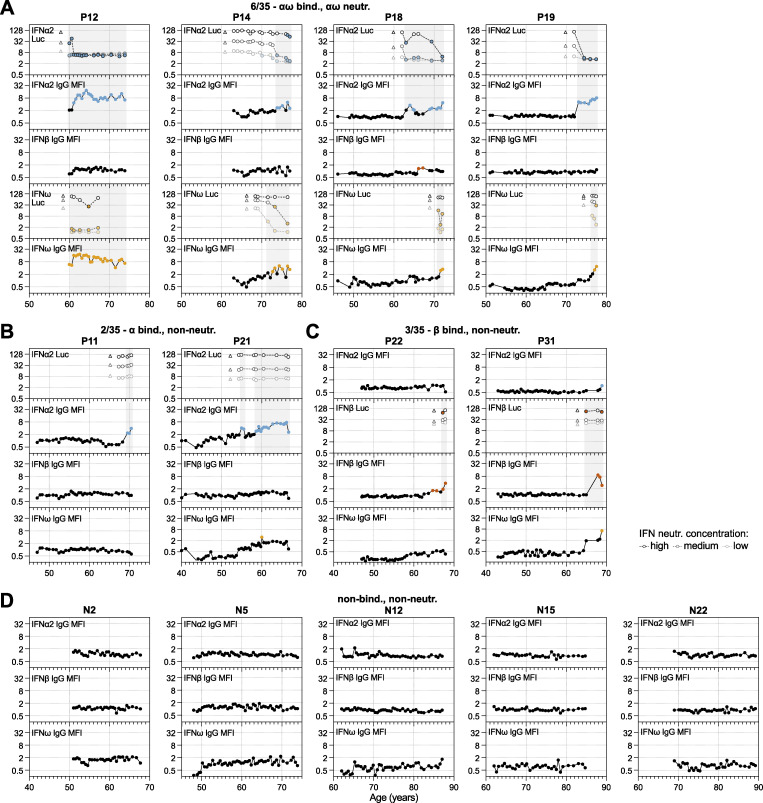
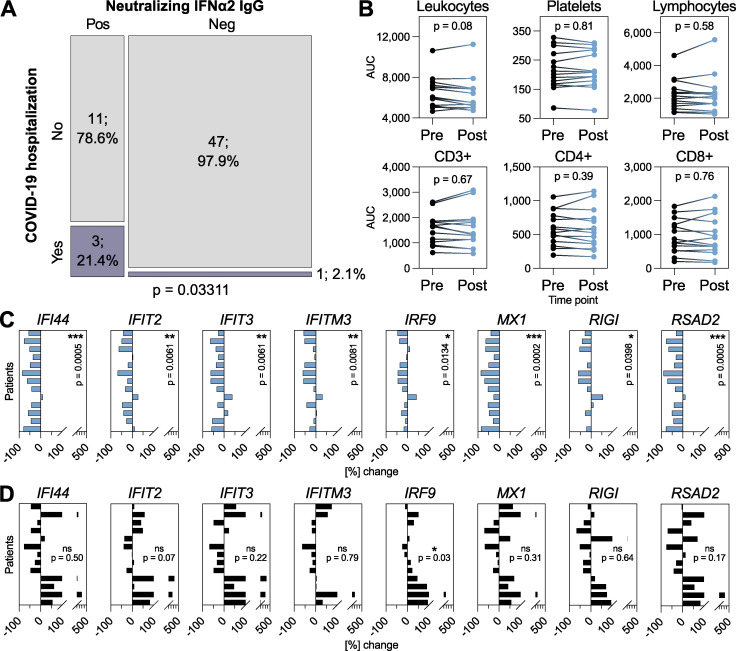
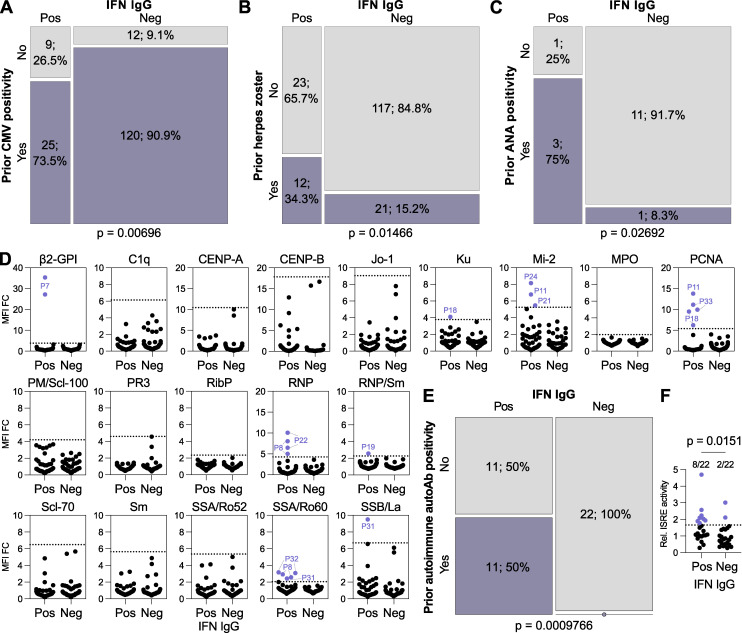
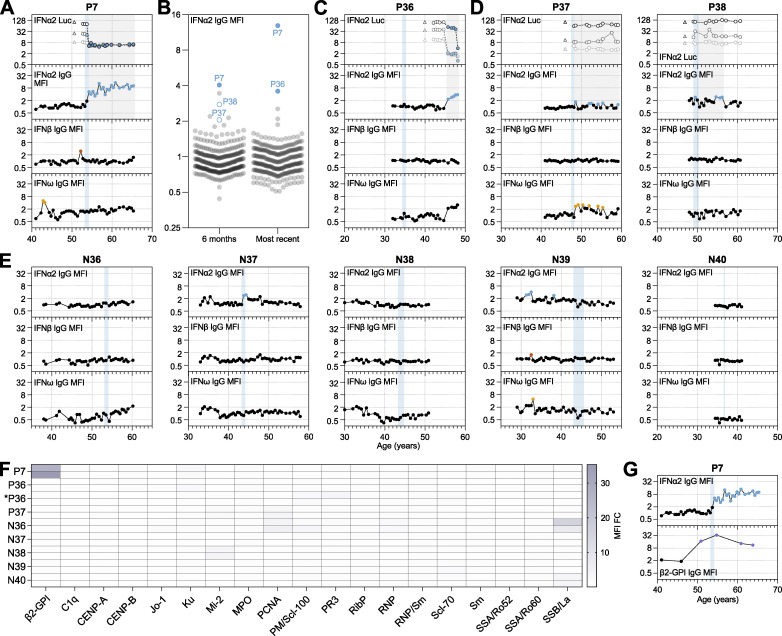
Autoantibodies neutralizing type I interferons (IFN-Is) can underlie infection severity. Here, we trace the development of these autoantibodies at high-resolution using longitudinal samples from 1,876 well-treated individuals living with HIV over a 35-year period. Similar to general populations, ∼1.9% of individuals acquired anti-IFN-I autoantibodies as they aged (median onset ∼63 years). Once detected, anti-IFN-I autoantibodies persisted lifelong, and titers increased over decades. Individuals developed distinct neutralizing and non-neutralizing autoantibody repertoires at discrete times that selectively targeted combinations of IFNα, IFNβ, and IFNω. Emergence of neutralizing anti-IFNα autoantibodies correlated with reduced baseline IFN-stimulated gene levels and was associated with subsequent susceptibility to severe COVID-19 several years later. Retrospective measurements revealed enrichment of pre-existing autoreactivity against other autoantigens in individuals who later developed anti-IFN-I autoantibodies, and there was evidence for prior viral infections or increased IFN at the time of anti-IFN-I autoantibody triggering. These analyses suggest that age-related loss of self-tolerance prior to IFN-I immune-triggering poses a risk of developing lifelong functional IFN-I deficiency.
© 2024 Fernbach et al.
Conflict of interest statement
Disclosures: E. Bernasconi reported grants from the Swiss National Science Foundation during the conduct of the study, grants from Merck outside the submitted work, and reported that his institution received fees for his participation to advisory boards and travel grants from Merck, Gilead Sciences, ViiV Healthcare, Pfizer AG Switzerland, Moderna, Astra Zeneca, Abbvie, and Ely Lilly. J. Notter reported travel grant/conference attendance paid by Gilead. A. Rauch reported support to his institution for advisory boards and/or travel grants from MSD, Gilead Sciences, Pfizer, and Moderna, and an investigator-initiated trial (IIT) grant from Gilead Sciences. All remuneration went to his home institution and not to A. Rauch personally and all remuneration was provided outside the submitted work. H.F. Günthard reported grants from the Swiss National Science Foundation, NIH, Yvonne Jacob Foundation, Gilead Sciences, and ViiV Healthcare; personal fees from Merck, Gilead Sciences, GSK, Johnson and Johnson, Janssen, and Novartis, and grants from Bill and Melinda Gates Foundation outside the submitted work. R.D. Kouyos reported grants from Gilead Sciences, the Swiss National Science Foundation, and the National Institutes of Health outside the submitted work. No other disclosures were reported.
Figures
References
-
- Abers, M.S., Rosen L.B., Delmonte O.M., Shaw E., Bastard P., Imberti L., Quaresima V., Biondi A., Bonfanti P., Castagnoli R., et al. . 2021. Neutralizing type-I interferon autoantibodies are associated with delayed viral clearance and intensive care unit admission in patients with COVID-19. Immunol. Cell Biol. 99:917–921. 10.1111/imcb.12495 - DOI - PMC - PubMed
-
- Achleitner, M., Mair N.K., Dänhardt J., Kardashi R., Puhan M.A., Abela I.A., Toepfner N., de With K., Kanczkowski W., Jarzebska N., et al. . 2023. Absence of type I interferon autoantibodies or significant interferon signature alterations in adults with post-COVID-19 syndrome. Open Forum Infect. Dis. 11:ofad641. 10.1093/ofid/ofad641 - DOI - PMC - PubMed
-
- Akbil, B., Meyer T., Stubbemann P., Thibeault C., Staudacher O., Niemeyer D., Jansen J., Mühlemann B., Doehn J., Tabeling C., et al. . 2022. Early and rapid identification of COVID-19 patients with neutralizing type I interferon auto-antibodies. J. Clin. Immunol. 42:1111–1129. 10.1007/s10875-022-01252-2 - DOI - PMC - PubMed
-
- Alotaibi, F., Alharbi N.K., Rosen L.B., Asiri A.Y., Assiri A.M., Balkhy H.H., Al Jeraisy M., Mandourah Y., AlJohani S., Al Harbi S., et al. . 2023. Type I interferon autoantibodies in hospitalized patients with Middle East respiratory syndrome and association with outcomes and treatment effect of interferon beta-1b in MIRACLE clinical trial. Influenza Other Respir. Viruses. 17:e13116. 10.1111/irv.13116 - DOI - PMC - PubMed
-
- Babcock, B.R., Kosters A., Eddins D.J., Donaire M.S.B., Sarvadhavabhatla S., Pae V., Beltran F., Murray V.W., Gill G., Xie G., et al. . 2024. Transient anti-interferon autoantibodies in the airways are associated with efficient recovery from COVID-19. medRxiv. 10.1101/2024.01.11.24301000 (Preprint posted January 11, 2024). - DOI
