

Effectiveness of dexmedetomidine on patient-centred outcomes in surgical patients: a systematic review and Bayesian meta-analysis
- PMID: 39019769
- PMCID: PMC11347795
- DOI: 10.1016/j.bja.2024.06.007
Effectiveness of dexmedetomidine on patient-centred outcomes in surgical patients: a systematic review and Bayesian meta-analysis
Abstract
Background: Dexmedetomidine is increasingly used for surgical patients requiring general anaesthesia. However, its effectiveness on patient-centred outcomes remains uncertain. Our main objective was to evaluate the patient-centred effectiveness of intraoperative dexmedetomidine for adult patients requiring surgery under general anaesthesia.
Methods: We conducted a systematic search of MEDLINE, Embase, CENTRAL, Web of Science, and CINAHL from inception to October 2023. Randomised controlled trials (RCTs) comparing intraoperative use of dexmedetomidine with placebo, opioid, or usual care in adult patients requiring surgery under general anaesthesia were included. Study selection, data extraction, and risk of bias assessment were performed by two reviewers independently. We synthesised data using a random-effects Bayesian regression framework to derive effect estimates and the probability of a clinically important effect. For continuous outcomes, we pooled instruments with similar constructs using standardised mean differences (SMDs) and converted SMDs and credible intervals (CrIs) to their original scale when appropriate. We assessed the certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology. Our primary outcome was quality of recovery after surgery. To guide interpretation on the original scale, the Quality of Recovery-15 (QoR-15) instrument was used (range 0-150 points, minimally important difference [MID] of 6 points).
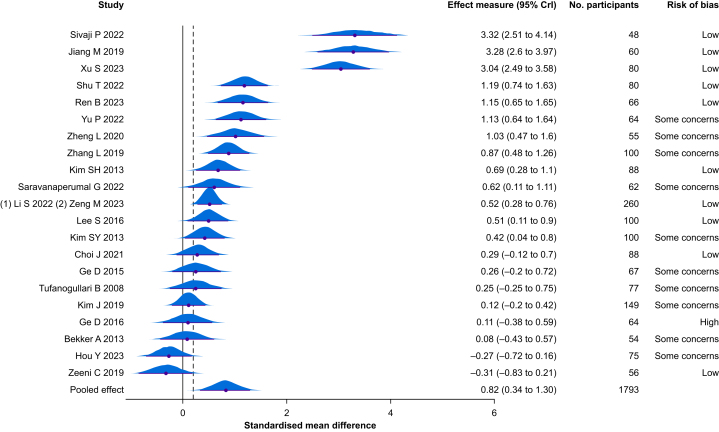
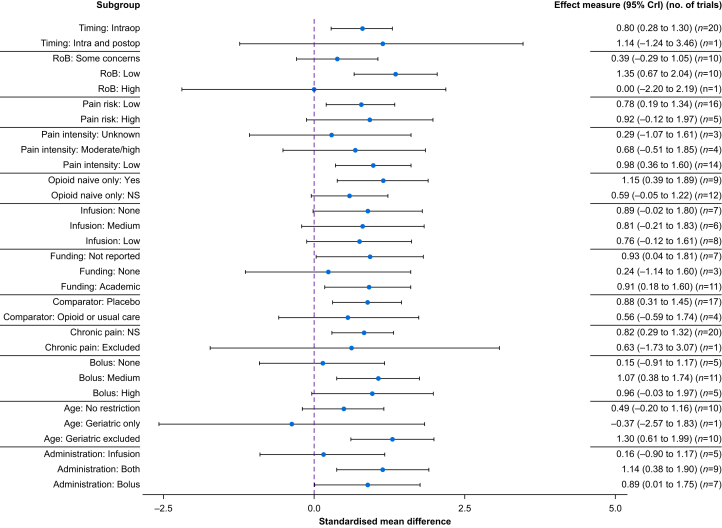
Results: We identified 49,069 citations, from which 44 RCTs involving 5904 participants were eligible. Intraoperative dexmedetomidine administration was associated with improvement in postoperative QoR-15 (mean difference 9, 95% CrI 4-14, n=21 RCTs, moderate certainty of evidence). We found 99% probability of any benefit and 88% probability of achieving the MID. There was a reduction in chronic pain incidence (odds ratio [OR] 0.42, 95% CrI 0.19-0.79, n=7 RCTs, low certainty of evidence). There was also increased risk of clinically significant hypotension (OR 1.98, 95% CrI 0.84-3.92, posterior probability of harm 94%, n=8 RCTs) and clinically significant bradycardia (OR 1.74, 95% CrI 0.93-3.34, posterior probability of harm 95%, n=10 RCTs), with very low certainty of evidence for both. There was limited evidence to inform other secondary patient-centred outcomes.
Conclusions: Compared with placebo or standard of care, intraoperative dexmedetomidine likely results in meaningful improvement in the quality of recovery and chronic pain after surgery. However, it might increase clinically important bradycardia and hypotension.
Systematic review protocol: PROSPERO (CRD42023439896).
Keywords: adult anaesthesia; chronic postsurgical pain; clinical pharmacology; dexmedetomidine; opioid minimisation strategies; pain management; patient-centred outcomes.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
IG has received consulting fees from GW Research, Eupraxia, Biogen, and Novaremed. The other authors have no conflict of interest to declare.
Figures

References
-
- Paranjpe J.S. Dexmedetomidine: expanding role in anesthesia. Med J Dr D Y Patil Univ. 2013;6:5–13.
-
- Precedex Approval Letter. In: Administration USoAFaD, ed. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/99/21-038_Precedex_Ap.... [Accessed 30 June 2023].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
