

Biomarkers in pulmonary infections: a clinical approach
- PMID: 39020244
- PMCID: PMC11254884
- DOI: 10.1186/s13613-024-01323-0
Biomarkers in pulmonary infections: a clinical approach
Abstract
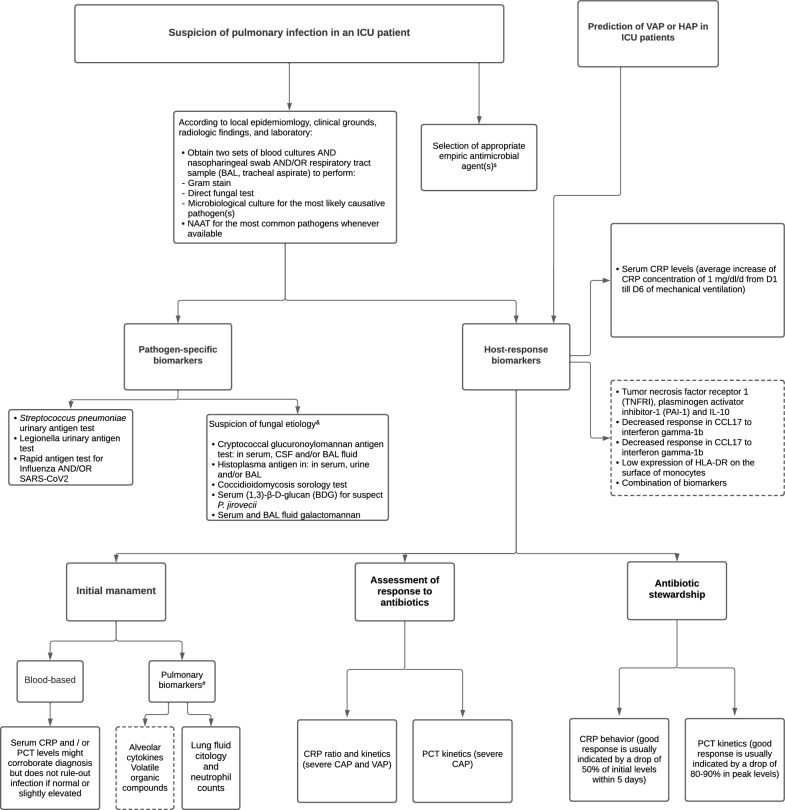
Severe acute respiratory infections, such as community-acquired pneumonia, hospital-acquired pneumonia, and ventilator-associated pneumonia, constitute frequent and lethal pulmonary infections in the intensive care unit (ICU). Despite optimal management with early appropriate empiric antimicrobial therapy and adequate supportive care, mortality remains high, in part attributable to the aging, growing number of comorbidities, and rising rates of multidrug resistance pathogens. Biomarkers have the potential to offer additional information that may further improve the management and outcome of pulmonary infections. Available pathogen-specific biomarkers, for example, Streptococcus pneumoniae urinary antigen test and galactomannan, can be helpful in the microbiologic diagnosis of pulmonary infection in ICU patients, improving the timing and appropriateness of empiric antimicrobial therapy since these tests have a short turnaround time in comparison to classic microbiology. On the other hand, host-response biomarkers, for example, C-reactive protein and procalcitonin, used in conjunction with the clinical data, may be useful in the diagnosis and prediction of pulmonary infections, monitoring the response to treatment, and guiding duration of antimicrobial therapy. The assessment of serial measurements overtime, kinetics of biomarkers, is more informative than a single value. The appropriate utilization of accurate pathogen-specific and host-response biomarkers may benefit clinical decision-making at the bedside and optimize antimicrobial stewardship.
Keywords: C-reactive protein; Host-response biomarkers; Pathogen-specific biomarkers; Procalcitonin; Pulmonary infections.
© 2024. The Author(s).
Conflict of interest statement
PP Lectures: Gilead, Pfizer, Mundipharma, MSD and Advisory board: Biocodex, Gilead; ACM Lectures: Thermo-Fisher, Biomerieux, Fischer and Paykel and Boston Scientific and Advisory board: Cambridge Infection Diagnostics; supported by an MRC Clinician Scientist Fellowship (MR/V006118/1); SN Lectures and Advisory Board: Pfizer, MSD, Biomérieux, Mundi Pharma, Medtronic, Fisher and Peykel; IML Lectures: Gilead, Thermofisher, Pfizer, MSD, Menarini and Advisory board: Fresenius Kabi, Advanz Pharma, Gilead, Accelerate, MSD; PR Lectures: Pfizer, MSD, Gilead, Novartis, Shionogi; AR Lectures: MSD, Gilead, Mundipharma; LC, JPC, AC, JS, VN, TL, DAS, ACK declare no COI.
Figures
References
-
- Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociacion Latinoamericana del Torax (ALAT) Eur Respir J. 2017 doi: 10.1183/13993003.00582-2017. - DOI - PubMed
-
- Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61–e111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
