

Maternal mortality due to obstetric hemorrhage by surgical injury during cesarean section: A nationwide study
- PMID: 39021333
- PMCID: PMC11324917
- DOI: 10.1111/aogs.14917
Maternal mortality due to obstetric hemorrhage by surgical injury during cesarean section: A nationwide study
Abstract
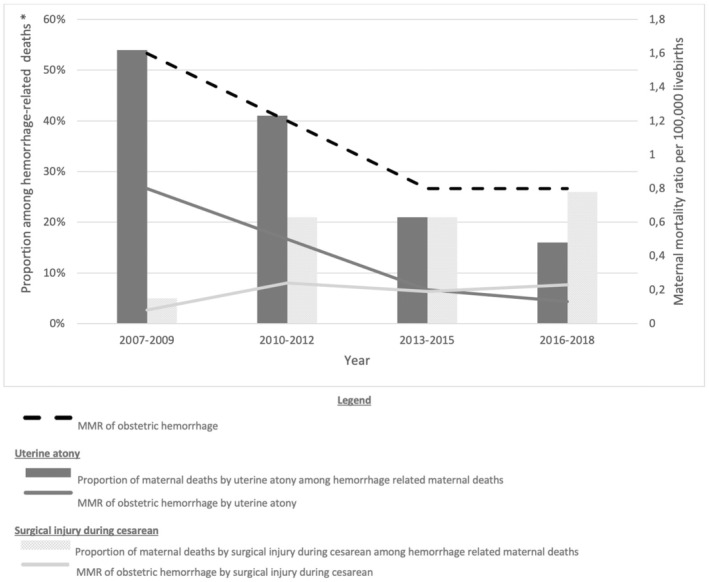
Introduction: Obstetric hemorrhage remains a largely preventable cause of maternal mortality globally. The contribution of uterine atony to hemorrhage-related maternal mortality has decreased in France, while the contribution of other causes of obstetric hemorrhage such as surgical injury during cesarean has been reported to increase. However, little evidence exists regarding the risk factors and care processes of women who died from this cause of hemorrhage. Therefore, we aimed to describe the clinical profile, underlying mechanisms, and preventability factors among women who died from obstetric hemorrhage by surgical injury during cesarean section.
Material and methods: Nationwide analysis of all hemorrhage-related maternal deaths by surgical injury during cesarean in France identified by the nationwide permanent enhanced maternal mortality surveillance system (ENCMM) between 2007 and 2018. We described the characteristics of the women, delivery hospitals, circumstances of hemorrhage, features of obstetric and resuscitation/transfusion care, and main preventability factors.
Results: Between 2007 and 2018, hemorrhage-related maternal mortality in France decreased from 1.6/100 000 live births (95% CI 1.1-2.2) (39/2 472 650) in 2007-2009 to 0.8/100 000 live births (95% CI 0.5-1.3) (19/2 311 783) in 2016-2018. Hemorrhage-related maternal mortality ratio due to surgical injury during cesarean increased from 0.08 (95% CI 0.01-0.3) (2/2 472 650) to 0.2 (95% CI 0.07-0.5) (5/2 311 783) per 100 000 live births. Among the 18 women who died from surgical injury during cesarean over the 12-year study period, we report a high prevalence of obesity (67%, 12/18), previous cesarean (72%, 13/18), and second-stage cesareans (56%, 10/18). In 22% (4/18), cesarean section was performed in a hospital providing <1000 births annually, with no blood bank (39%, 7/18) or no adult intensive care (44%, 8/18) on-site. Overall preventability of deaths was 94% (17/18). Main preventability factors were related to delay in hemorrhage diagnosis (77%, 14/18) due to late recognition of abnormal parameters (33%, 6/18) and late bedside ultrasound (56%, 10/18), and delay in management due to insufficient surgical skills (56%, 10/18).
Conclusions: In France, surgical injury during cesarean section is an increasing, largely preventable contributor to hemorrhage-related maternal mortality, as other causes of fatal hemorrhage have become less frequent. The profile of these women showed a high prevalence of obesity, previous cesarean, second-stage cesarean, and delivery in hospitals with limited medical and surgical resources, which suggests explanatory mechanisms for the fatal outcome and opportunities for prevention.
Keywords: cesarean section; cesarean surgical injury; maternal mortality; obstetric hemorrhage; postpartum hemorrhage; preventability factors; severe maternal outcome; surgical trauma.
© 2024 The Author(s). Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None.
Figures
References
-
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323‐e333. - PubMed
-
- Lepine SJ, Geller SE, Pledger M, Lawton B, MacDonald EJ. Severe maternal morbidity due to obstetric haemorrhage: potential preventability. Aust N Z J Obstet Gynaecol. 2020;60:212‐217. - PubMed
-
- Della Torre M, Kilpatrick SJ, Hibbard JU, et al. Assessing preventability for obstetric hemorrhage. Am J Perinatol. 2011;28:753‐760. - PubMed
-
- World Health Organization . A Roadmap to combat postpartum haemorrhage between 2023 and 2030. Licence: CC BY‐NC‐SA 3.0 IGO; 2023. Disponible surhttps://iris.who.int/bitstream/handle/10665/373221/9789240081802‐eng.pdf...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
