

Urinary soluble CD163 is useful as "liquid biopsy" marker in lupus nephritis at both diagnosis and follow-up to predict impending flares
- PMID: 39021518
- PMCID: PMC11253685
- DOI: 10.1016/j.jtauto.2024.100244
Urinary soluble CD163 is useful as "liquid biopsy" marker in lupus nephritis at both diagnosis and follow-up to predict impending flares
Abstract
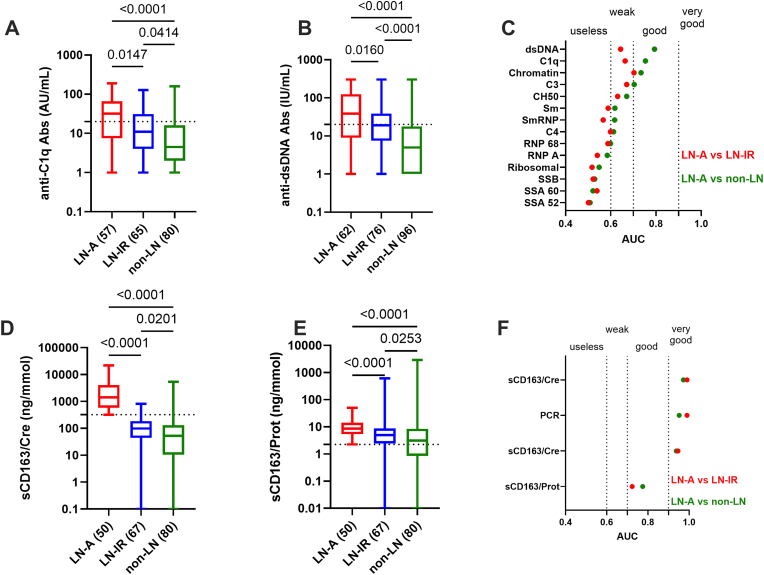
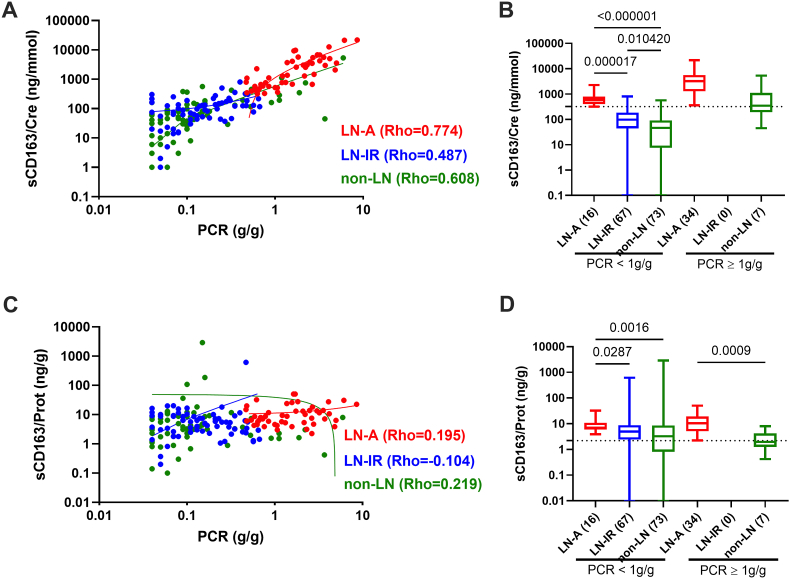
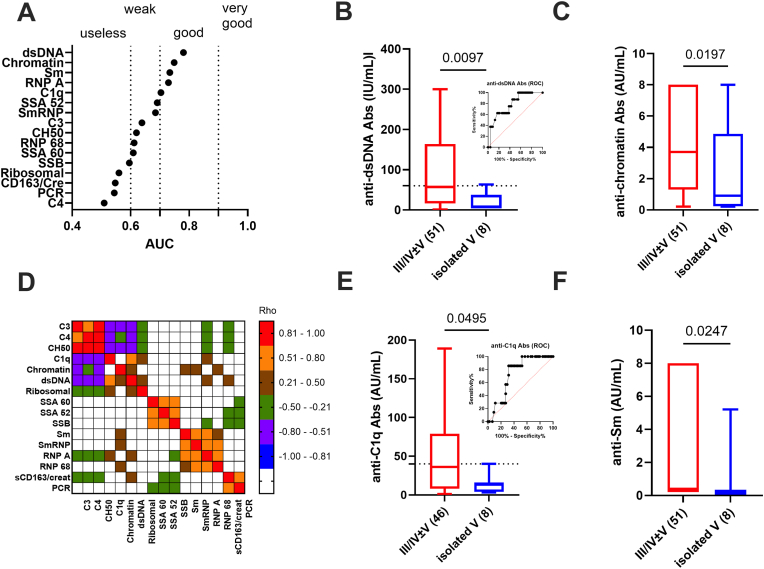
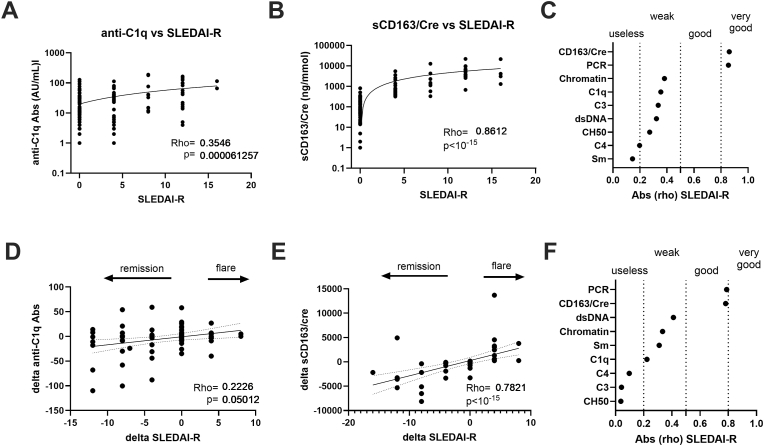
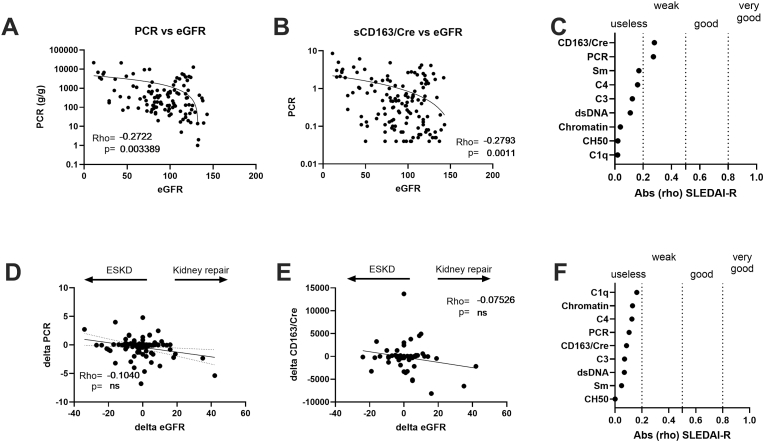
Lupus nephritis (LN) diagnosis and follow-up requires noninvasive biomarkers. Therefore, the added value of coupling the urinary soluble (s)CD163/creatinuria ratio with serological markers was evaluated in a real-world clinical practice. To this end, a monocentric and retrospective study was conducted in 139 SLE patients with biopsy-proven nephritis having an active LN (LN-A, n = 63 with a positive SLEDAI-renal score) or inactive (n = 76), as well as 98 non-renal SLE patients. The urinary sCD163/creatinuria ratio outperformed serological markers for predicting LN-A (AUC>0.972; p < 10-4 with a 100 % specificity threshold fixed at 320 ng/mmol), and for monitoring renal activity allowing prediction of impending flares and remissions in follow-up (AUC = 0.789, p < 10-4). LN-A patients with an elevated spot proteinuria/creatinuria ratio (p = 8 × 10-6) and sCD163/creatinuria ratio (p = 10-3) were at risk for developing end-stage kidney disease but sCD163/creatinuria ratio cannot substitute kidney biopsy to discriminate LN-A from other glomerulonephritis. Among serological markers (n = 14), anti-dsDNA and anti-C1q antibodies (Abs) (AUC>0.750 versus non-LN patients, and AUC>0.640 versus LN-IR patients) best predicted LN-A, and higher levels were retrieved in class III/IV proliferative LN-A. In multivariate logistic regression analysis, the urinary sCD163/creatinuria ratio remained the only statistically significant biomarker to predict LN-A (p < 0.001). In conclusion, and as compared to classical serological markers, the urinary sCD163/creatinuria ratio provides an additional parameter for monitoring LN patients.
Keywords: Biomarkers; End stage kidney disease; Flare; Remission; Urinary soluble CD163; lupus nephritis.
© 2024 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Anders H.J., et al. Lupus nephritis. Nat. Rev. Dis. Prim. 2020;6(1):7. - PubMed
-
- Bajema I.M., et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018;93(4):789–796. - PubMed
-
- Fernandes das Neves M., Irlapati R.V., Isenberg D. Assessment of long-term remission in lupus nephritis patients: a retrospective analysis over 30 years. Rheumatology. 2015;54(8):1403–1407. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
