

Case report: A patient with brachio-cervical inflammatory myopathy was misdiagnosed as flail arm syndrome
- PMID: 39021570
- PMCID: PMC11251991
- DOI: 10.3389/fimmu.2024.1378130
Case report: A patient with brachio-cervical inflammatory myopathy was misdiagnosed as flail arm syndrome
Abstract
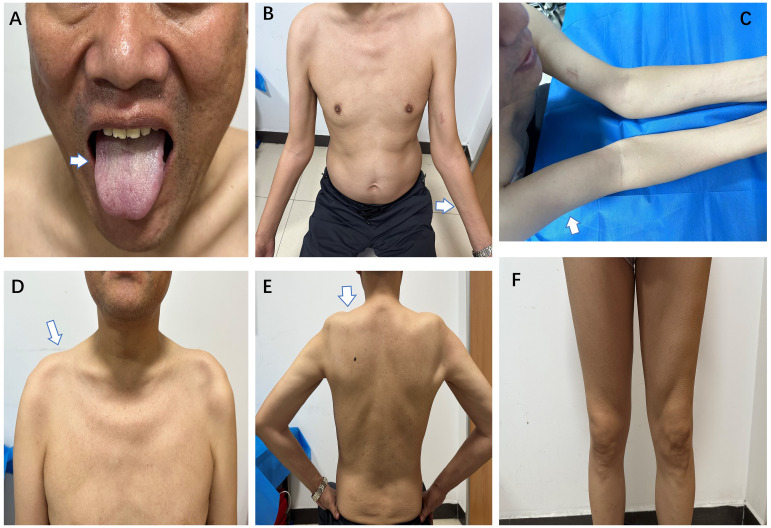
Brachio-cervical inflammatory myopathy (BCIM) is a rare inflammatory myopathy characterized by dysphagia, bilateral upper limb atrophy, limb-girdle muscle weakness, and myositis-specific antibody (MSA) negativity. BCIM has a low incidence and is commonly associated with autoimmune diseases. We present a case report of a 55-year-old man with progressive upper limb weakness and atrophy, diagnosed with flail arm syndrome (FAS). The initial electromyography revealed extensive spontaneous muscle activity and increased duration of motor unit potentials (MUPs). During follow-up, evidence of myogenic damage was observed, as indicated by a decreased duration of MUPs in the right biceps muscle. Laboratory and genetic testing ruled out hereditary or acquired diseases. Negative serological antibodies for myasthenia gravis. Hereditary or acquired diseases were ruled out through laboratory and genetic testing. Whole-body muscle magnetic resonance imaging (MRI) showed extensive edema and fat replacement in the bilateral upper limbs, scapular, and central axis muscles, while the lower extremities were relatively mildly affected. Muscle biopsy revealed numerous foci of inflammatory cells distributed throughout the muscle bundle, with predominant CD20, CD138, and CD68 expression, accompanied by a light infiltration of CD3 and CD4 expression. The muscle weakness improved with the combination of oral prednisone (initially 60 mg/day, tapered) and methotrexate (5 mg/week) treatment.
Keywords: brachio-cervical inflammatory myopathy; case report; flail arm syndrome; misdiagnosis; myositis.
Copyright © 2024 Sun, Wei, Han, Wang, Wang and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Van der Kooi A, Jaeger B, Pinto Y, Aronica E, de Visser M. Two women with brachio-cervical inflammatory myopathy (BCIM) and fatal cardiomyopathy. Neuromuscular Disord. (2015) 25(Supplement 2):S308. doi: 10.1016/j.nmd.2015.06.435 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous