

A nomogram for risk stratification of central cervical lymph node metastasis in patients with papillary thyroid carcinoma
- PMID: 39022275
- PMCID: PMC11250316
- DOI: 10.21037/qims-24-284
A nomogram for risk stratification of central cervical lymph node metastasis in patients with papillary thyroid carcinoma
Abstract
Background: Whether to perform prophylactic central lymph node dissection for cN0 papillary thyroid carcinoma (PTC) patients is still controversial. This retrospective study aimed to develop and validate a nomogram based on ultrasound and dual-energy computed tomography (DECT) for the risk stratification of central lymph node metastasis (CLNM) in patients with PTC.
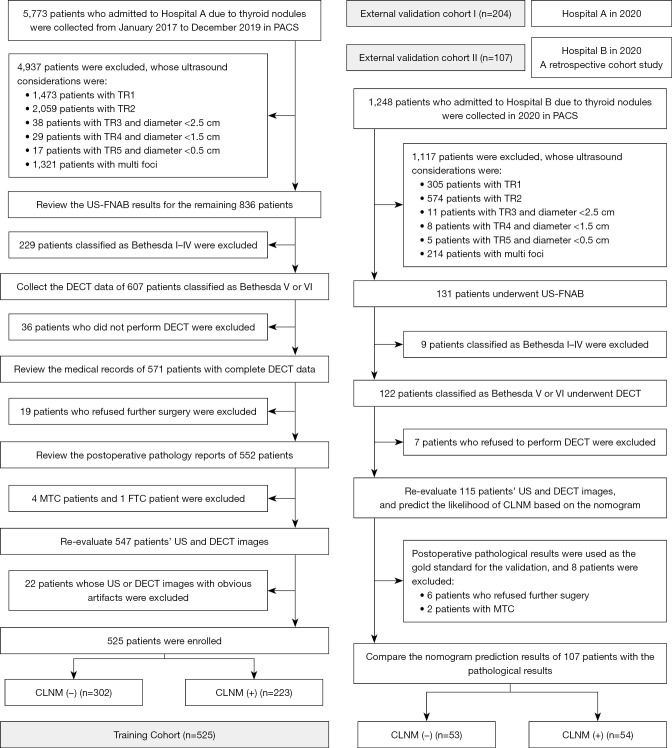
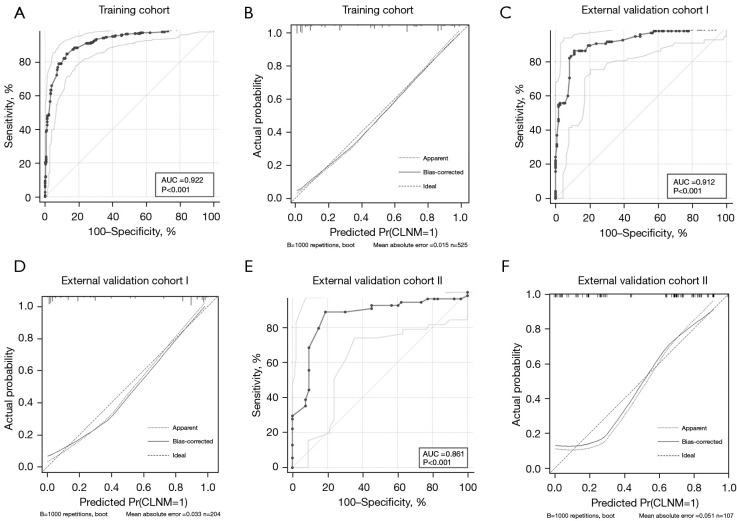
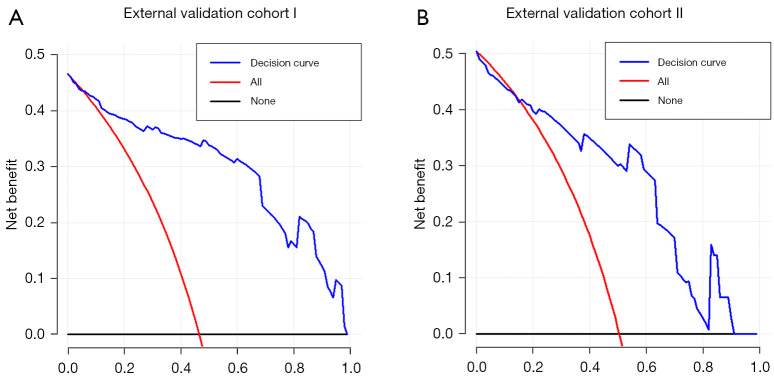
Methods: A total of 525 patients from 2017 to 2019 [Tianjin First Central Hospital (Hospital A)] were retrospectively analyzed to form the training cohort and to conduct internal validation. Another group of 204 patients in 2020 (Hospital A) formed the temporal validation cohort. A total of 107 patients in 2020 [Binzhou Medical University Hospital (Hospital B)] formed the geographic validation cohort, which was a retrospective cohort study. The area under the curve (AUC), calibration curve, and decision curve were used to evaluate the performance of the nomogram. The locally weighted regression curve was used for risk stratification.
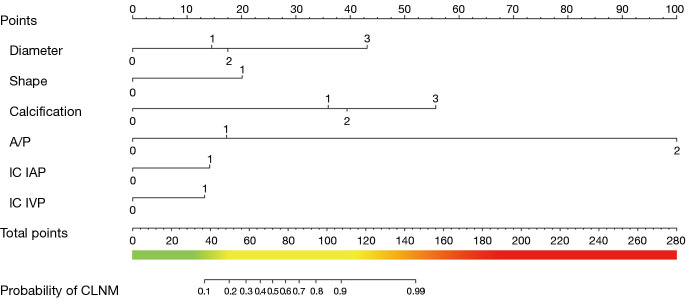
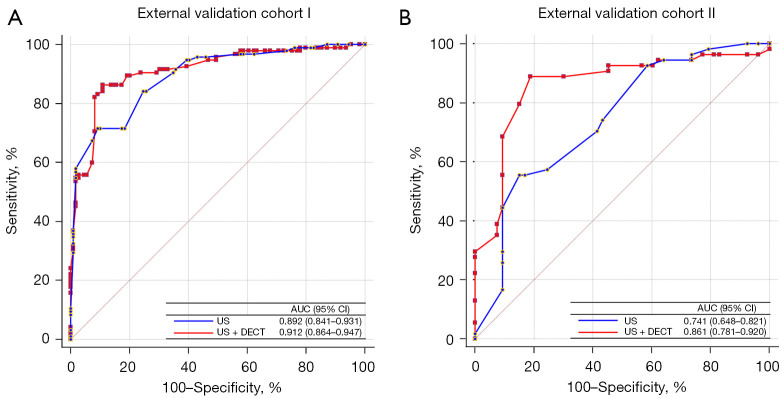
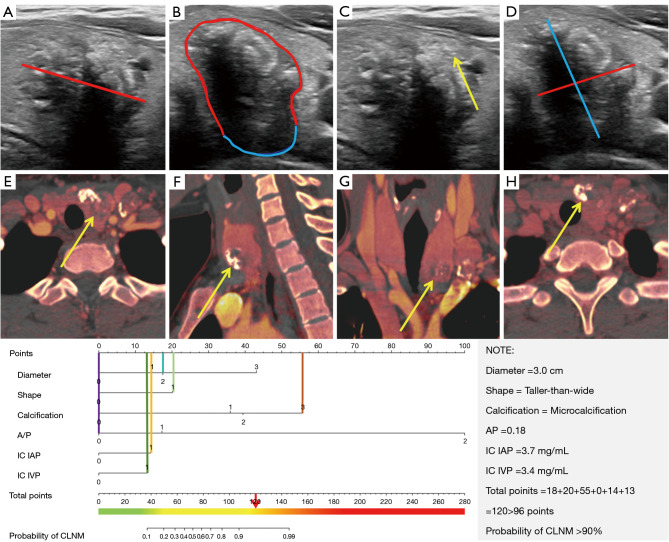
Results: Diameter, taller-than-wide, calcification, capsular invasion, and iodine concentration in the arterial and venous phases were independent risk predictors of CLNM. The AUC of the nomogram was 0.922 (95% confidence interval: 0.895-0.943) in the training cohort. Two external validation cohorts demonstrated the good performance of the nomogram in predicting CLNM, with AUCs of 0.912 and 0.861. The significantly improved net reclassification index and integrated discriminatory improvement index indicated that DECT was a powerful supplement to ultrasound for predicting CLNM. The risk stratification system divided all patients into low-risk (0-50 points), intermediate-risk (51-100 points), and high-risk groups (>100 points).
Conclusions: The nomogram and risk stratification system estimated the utility of CLNM to guide individualized treatment of patients with PTC.
Keywords: Papillary thyroid carcinoma (PTC); dual-energy computed tomography (DECT); lymphatic metastasis; nomogram; risk assessment.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-24-284/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Development and validation of a dynamic nomogram for predicting central lymph node metastasis in papillary thyroid carcinoma patients based on clinical and ultrasound features.Quant Imaging Med Surg. 2025 Feb 1;15(2):1555-1570. doi: 10.21037/qims-24-618. Epub 2025 Jan 22. Quant Imaging Med Surg. 2025. PMID: 39995718 Free PMC article.
-
Prediction model construction of cervical central lymph node metastasis in papillary thyroid carcinoma combined with Hashimoto's thyroiditis utilizing conventional ultrasound and elastography.Gland Surg. 2024 Dec 31;13(12):2325-2334. doi: 10.21037/gs-24-271. Epub 2024 Dec 27. Gland Surg. 2024. PMID: 39822354 Free PMC article.
-
Preoperative prediction of central lymph node metastasis in cN0T1/T2 papillary thyroid carcinoma: A nomogram based on clinical and ultrasound characteristics.Eur J Surg Oncol. 2022 Jun;48(6):1272-1279. doi: 10.1016/j.ejso.2022.04.001. Epub 2022 Apr 6. Eur J Surg Oncol. 2022. PMID: 35414404
-
A nomogram for enhanced risk stratification for predicting cervical lymph node metastasis in papillary thyroid carcinoma patients.Discov Oncol. 2024 Sep 27;15(1):476. doi: 10.1007/s12672-024-01370-w. Discov Oncol. 2024. PMID: 39331286 Free PMC article.
-
The diagnostic performance of dual-energy CT imaging in cervical lymph node metastasis of papillary thyroid cancer: a meta-analysis.Front Med (Lausanne). 2024 Nov 6;11:1457307. doi: 10.3389/fmed.2024.1457307. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39568751 Free PMC article. Review.
Cited by
-
Development and validation of a dynamic nomogram for predicting central lymph node metastasis in papillary thyroid carcinoma patients based on clinical and ultrasound features.Quant Imaging Med Surg. 2025 Feb 1;15(2):1555-1570. doi: 10.21037/qims-24-618. Epub 2025 Jan 22. Quant Imaging Med Surg. 2025. PMID: 39995718 Free PMC article.
-
Prediction model construction of cervical central lymph node metastasis in papillary thyroid carcinoma combined with Hashimoto's thyroiditis utilizing conventional ultrasound and elastography.Gland Surg. 2024 Dec 31;13(12):2325-2334. doi: 10.21037/gs-24-271. Epub 2024 Dec 27. Gland Surg. 2024. PMID: 39822354 Free PMC article.
References
-
- Carling T, Carty SE, Ciarleglio MM, Cooper DS, Doherty GM, Kim LT, Kloos RT, Mazzaferri EL, Sr, Peduzzi PN, Roman SA, Sippel RS, Sosa JA, Stack BC, Jr, Steward DL, Tufano RP, Tuttle RM, Udelsman R; . American Thyroid Association design and feasibility of a prospective randomized controlled trial of prophylactic central lymph node dissection for papillary thyroid carcinoma. Thyroid 2012;22:237-44. 10.1089/thy.2011.0317 - DOI - PubMed
LinkOut - more resources
Full Text Sources