

Imaging modalities for characterising T1 renal tumours: A systematic review and meta-analysis of diagnostic accuracy
- PMID: 39022655
- PMCID: PMC11249832
- DOI: 10.1002/bco2.355
Imaging modalities for characterising T1 renal tumours: A systematic review and meta-analysis of diagnostic accuracy
Erratum in
-
Erratum.BJUI Compass. 2024 Dec 30;5(12):1324-1329. doi: 10.1002/bco2.482. eCollection 2024 Dec. BJUI Compass. 2024. PMID: 39744071 Free PMC article.
Abstract
Objectives: International guidelines recommend resection of suspected localised renal cell carcinoma (RCC), with surgical series showing benign pathology in 30%. Non-invasive diagnostic tests to differentiate benign from malignant tumours are an unmet need. Our objective was to determine diagnostic accuracy of imaging modalities for detecting cancer in T1 renal tumours.
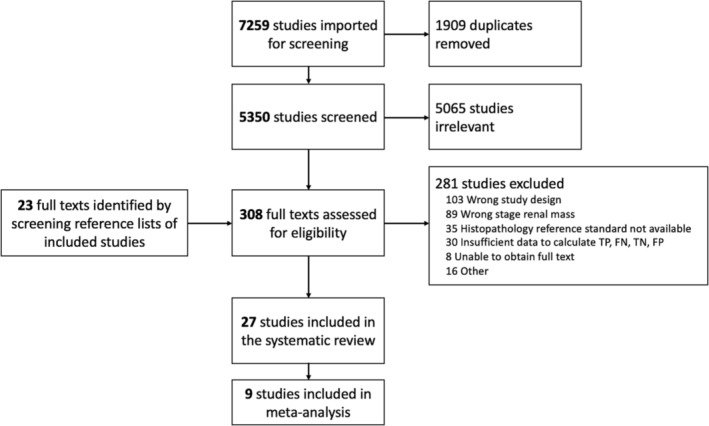
Methods: A systematic review was performed for reports of diagnostic accuracy of any imaging test compared to a reference standard of histopathology for T1 renal masses, from inception until January 2023. Twenty-seven publications (including 2277 tumours in 2044 participants) were included in the systematic review, and nine in the meta-analysis.
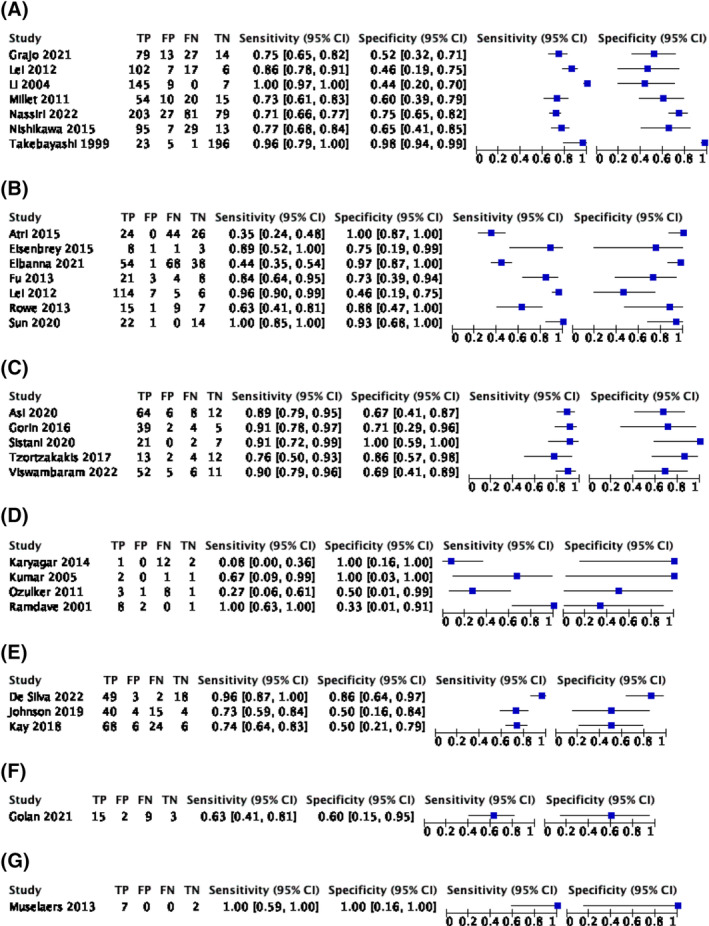
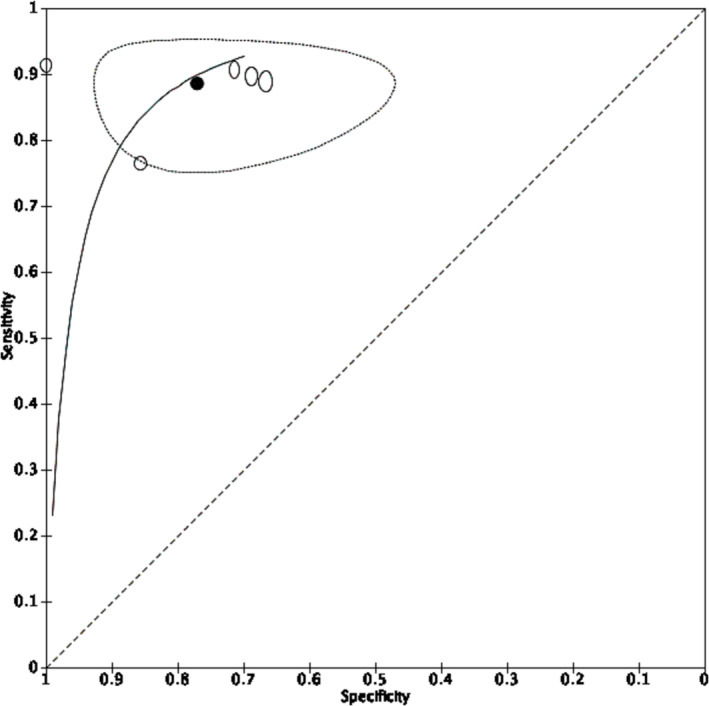
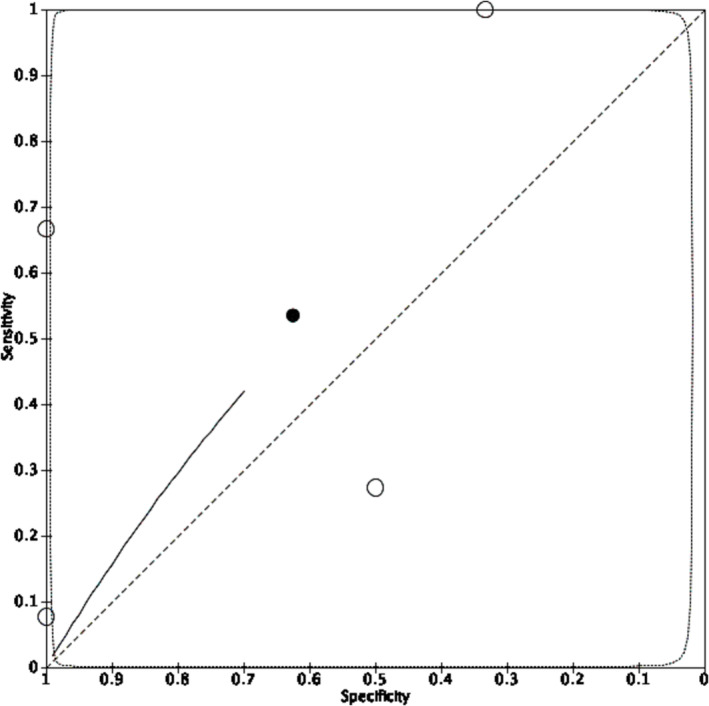
Results: Forest plots of sensitivity and specificity were produced for CT (seven records, 1118 participants), contrast-enhanced ultrasound (seven records, 197 participants), [99mTc]Tc-sestamibi SPECT/CT (five records, 263 participants), MRI (three records, 220 participants), [18F]FDG PET (four records, 43 participants), [68Ga]Ga-PSMA-11 PET (one record, 27 participants) and [111In]In-girentuximab SPECT/CT (one record, eight participants). Meta-analysis returned summary estimates of sensitivity and specificity for [99mTc]Tc-sestamibi SPECT/CT of 88.6% (95% CI 82.7%-92.6%) and 77.0% (95% CI 63.0%-86.9%) and for [18F]FDG PET 53.5% (95% CI 1.6%-98.8%) and 62.5% (95% CI 14.0%-94.5%), respectively. A comparison hierarchical summary receiver operating characteristic (HSROC) model did not converge. Meta-analysis was not performed for other imaging due to different thresholds for test positivity.
Conclusion: The optimal imaging strategy for T1 renal masses is not clear. [99mTc]Tc-sestamibi SPECT/CT is an emerging tool, but further studies are required to inform its role in clinical practice. The field would benefit from standardisation of diagnostic thresholds for CT, MRI and contrast-enhanced ultrasound to facilitate future meta-analyses.
Keywords: diagnostic accuracy; imaging; renal tumours.
© 2024 The Authors. BJUI Compass published by John Wiley & Sons Ltd on behalf of BJU International Company.
Conflict of interest statement
HW receives salary support from The Urology Foundation, Pan London Cancer Alliance (Royal Marsden Partners, North Central London Cancer Alliance, North East London Cancer Alliance, South East London Cancer Alliance and the NIHR BRCs) and the Wellcome/EPSRC Centre for Interventional and Surgical Sciences. The promotions and salaries of KG are dependent upon the publishing of research protocols and findings. Other authors have no relevant interests to declare.
Figures

References
-
- Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population‐based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. - PubMed
-
- Ljungberg B, Albiges L, Abu‐Ghanem Y, Bedke J, Capitanio U, Dabestani S, et al. European Association of Urology guidelines on renal cell carcinoma: the 2022 update. Eur Urol. 2022;82:399–410. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous