

Low-Density Lipoprotein Cholesterol, Cardiovascular Disease Risk, and Mortality in China
- PMID: 39023892
- PMCID: PMC11258592
- DOI: 10.1001/jamanetworkopen.2024.22558
Low-Density Lipoprotein Cholesterol, Cardiovascular Disease Risk, and Mortality in China
Abstract
Importance: Limited evidence supports the association between low-density lipoprotein cholesterol (LDL-C) and mortality across different atherosclerotic cardiovascular disease (ASCVD) risk stratifications.
Objective: To explore the associations between LDL-C levels and mortality and to identify the optimal ranges of LDL-C with the lowest risk of mortality in populations with diverse ASCVD risk profiles.
Design, setting, and participants: The ChinaHEART project is a prospective cohort study that recruited residents aged 35 to 75 years from 31 provinces in mainland China between November 2014 and December 2022. Participants were categorized into low-risk, primary prevention, and secondary prevention cohorts on the basis of their medical history and ASCVD risk. Data analysis was performed from December 2022 to October 2023.
Main outcomes and measures: The primary end point was all-cause mortality, and secondary end points included cause-specific mortality. Mortality data were collected from the National Mortality Surveillance System and Vital Registration. The association between LDL-C levels and mortality was assessed by using Cox proportional hazard regression models with various adjusted variables.
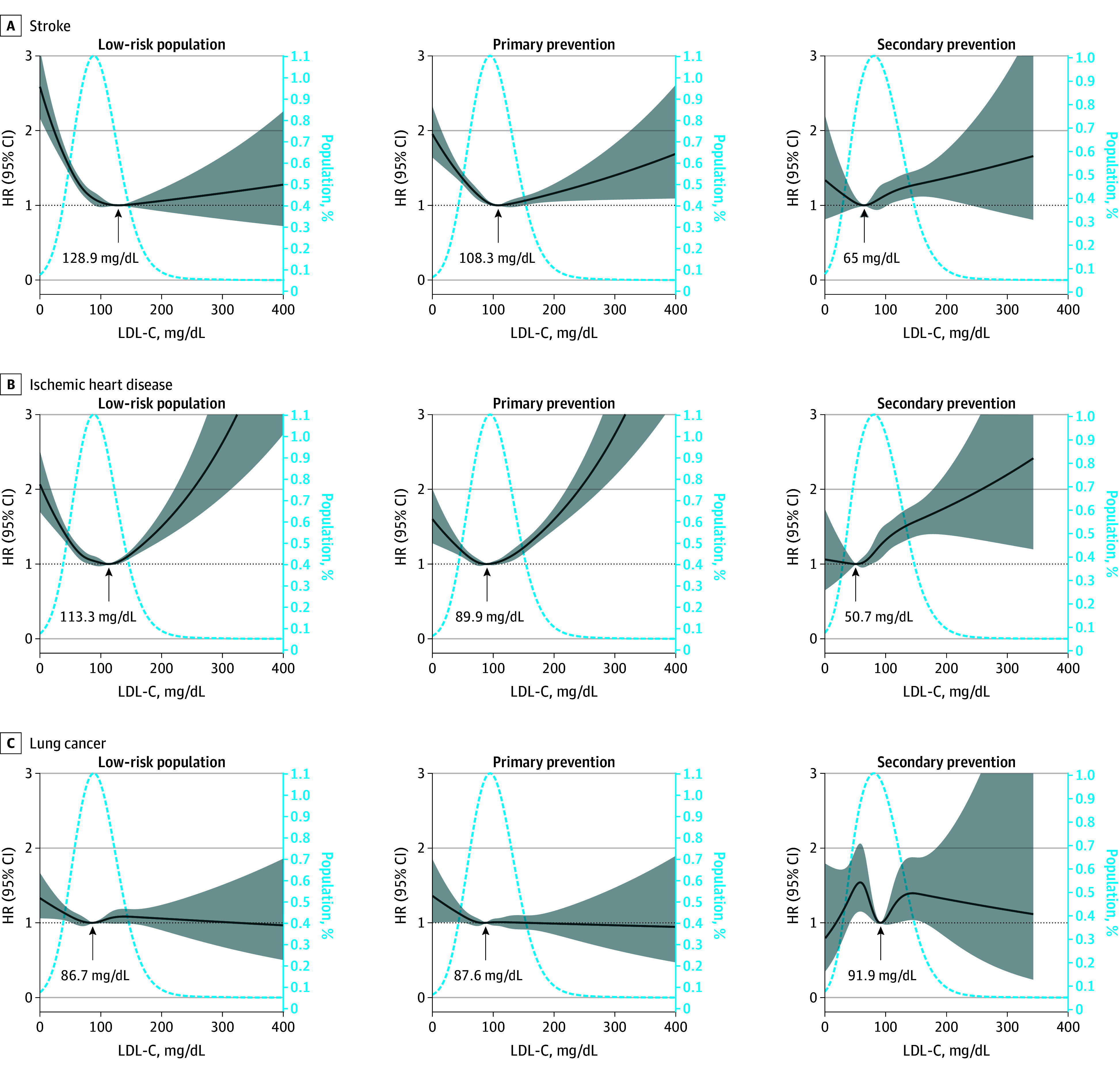
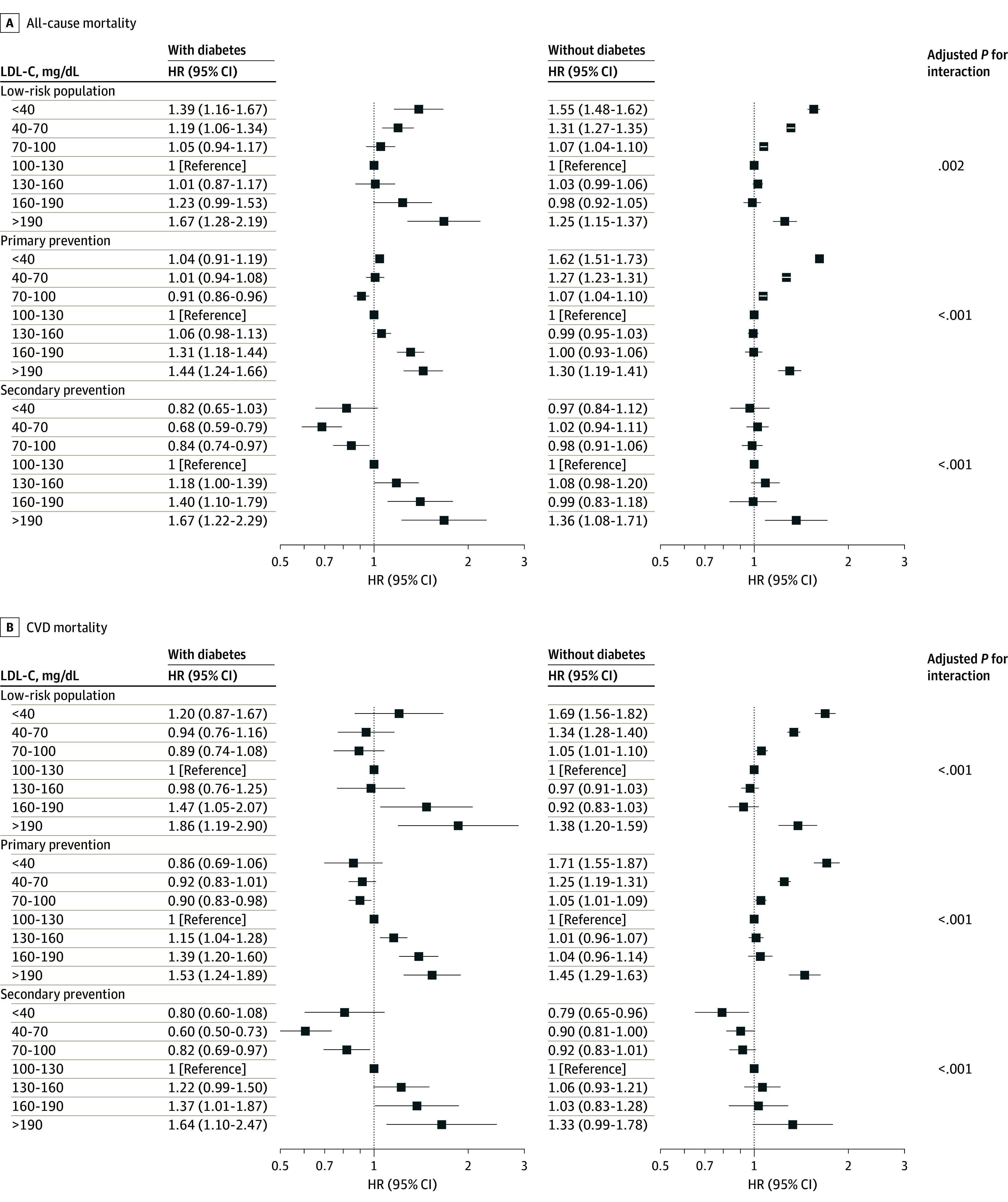
Results: A total of 4 379 252 individuals were recruited, and 3 789 025 (2 271 699 women [60.0%]; mean [SD] age, 56.1 [10.0] years) were included in the current study. The median (IQR) LDL-C concentration was 93.1 (70.9-117.3) mg/dL overall at baseline. During a median (IQR) follow-up of 4.6 (3.1-5.8) years, 92 888 deaths were recorded, including 38 627 cardiovascular deaths. The association between LDL-C concentration and all-cause or cardiovascular disease (CVD) mortality was U-shaped in both the low-risk cohort (2 838 354 participants) and the primary prevention cohort (829 567 participants), whereas it was J-shaped in the secondary prevention cohort (121 104 participants). The LDL-C levels corresponding to the lowest CVD mortality were 117.8 mg/dL in the low-risk group, 106.0 mg/dL in the primary prevention cohort, and 55.8 mg/dL in the secondary prevention cohort. The LDL-C concentration associated with the lowest all-cause mortality (90.9 mg/dL vs 117.0 mg/dL) and CVD mortality (87 mg/dL vs 114.6 mg/dL) were both lower in individuals with diabetes than in individuals without diabetes in the overall cohort.
Conclusions and relevance: This study found that the association between LDL-C and mortality varied among different ASCVD risk cohorts, suggesting that stricter lipid control targets may be needed for individuals with higher ASCVD risk and those with diabetes.
Conflict of interest statement
Figures


References
-
- Arnett DK, Blumenthal RS, Albert MA, et al. . 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646. doi:10.1161/CIR.0000000000000678 - DOI - PMC - PubMed
-
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2021;396(10267):2006-2017. doi:10.1016/S0140-6736(20)32340-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
