

Technique, Safety, and Accuracy Assessment of Percutaneous Pedicle Screw Placement Utilizing Computer-Assisted Navigation in Lateral Decubitus Single-Position Surgery
- PMID: 39025526
- PMCID: PMC11483630
- DOI: 10.14444/8613
Technique, Safety, and Accuracy Assessment of Percutaneous Pedicle Screw Placement Utilizing Computer-Assisted Navigation in Lateral Decubitus Single-Position Surgery
Abstract
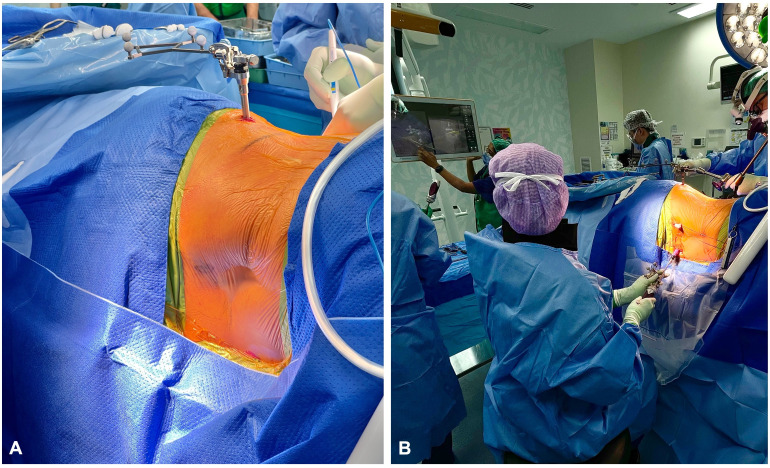
Background: Percutaneous pedicle screw (PPS) placement has become a pivotal technique in spinal surgery, increasing surgical efficiency and limiting the invasiveness of surgical procedures. The aim of this study was to analyze the accuracy of computer-assisted PPS placement with a standardized technique in the lateral decubitus position.
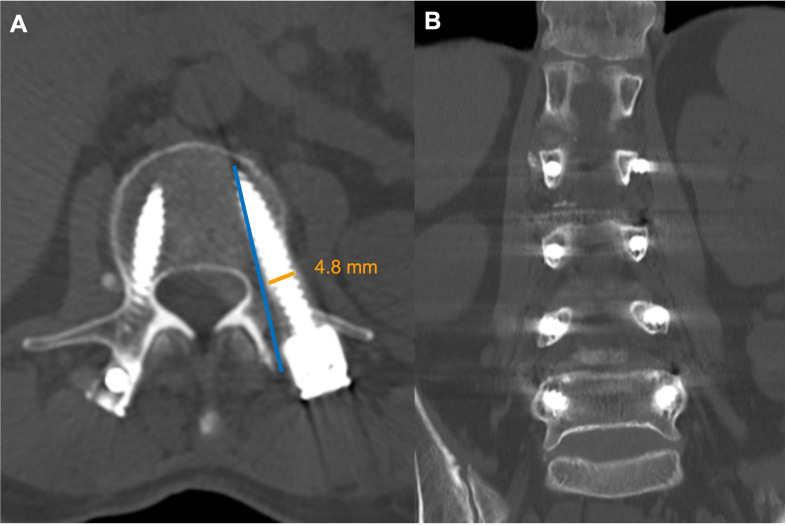
Methods: A retrospective review of prospectively collected data was performed on 44 consecutive patients treated between 2021 and 2023 with lateral decubitus single-position surgery. PPS placement was assessed by computed tomography scans, and breaches were graded based on the magnitude and direction of the breach. Facet joint violations were assessed. Variables collected included patient demographics, indication, intraoperative complications, operative time, fluoroscopy time, estimated blood loss, and length of stay.
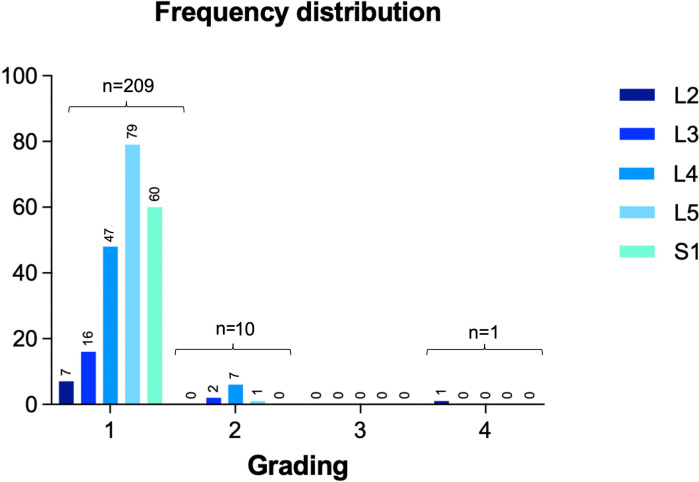
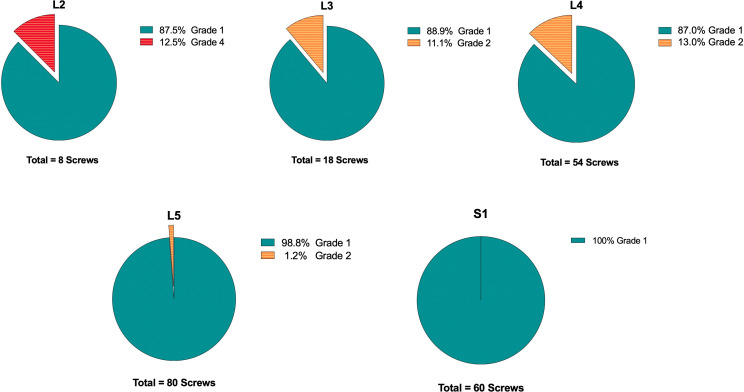
Results: Forty-four patients, with 220 PPSs were identified. About 79.5% of all patients underwent anterior lumbar interbody fusion only, 13.6% underwent lateral lumbar interbody fusion only, and 6.8% received a combination of both anterior lumbar interbody fusion and lateral lumbar interbody fusion. Eleven screw breaches (5%) were identified: 10 were Grade II breaches (<2 mm), and 1 was a Grade IV breach (>4 mm). All breaches were lateral. About 63.6% involved down-side screws indicating a trend toward the laterality of breaches for down-side pedicles. When analyzing breaches by level, 1.2% of screws at L5, 13% at L4, and 11.1% at L3 demonstrated Grade II breaches. No facet joint violations were noted.
Conclusion: PPS placement utilizing computer-assisted navigation in lateral decubitus single-position surgery is both safe and accurate. An overall breach rate of 5% was found; considering a safe zone of 2 mm, only 1 screw (0.5%) demonstrated a relevant breach.
Clinical relevance: PPS placement is both safe and accurate. Breaches are rare, and when breaches do occur, they are lateral.
Keywords: fusion; lateral decubitus; pedicle screw; percutaneous pedicle screw; single position surgery.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Figures

References
-
- Ouchida J, Kanemura T, Satake K, et al. . True accuracy of percutaneous pedicle screw placement in thoracic and lumbar spinal fixation with a CT-based navigation system: intraoperative and postoperative assessment of 763 percutaneous pedicle screws. J Clin Neurosci. 2020;79:1–6:S0967-5868(20)31349-7. 10.1016/j.jocn.2020.07.012 - DOI - PubMed
LinkOut - more resources
Full Text Sources