

Accelerated aging of skeletal muscle and the immune system in patients with chronic liver disease
- PMID: 39026032
- PMCID: PMC11297261
- DOI: 10.1038/s12276-024-01287-y
Accelerated aging of skeletal muscle and the immune system in patients with chronic liver disease
Abstract
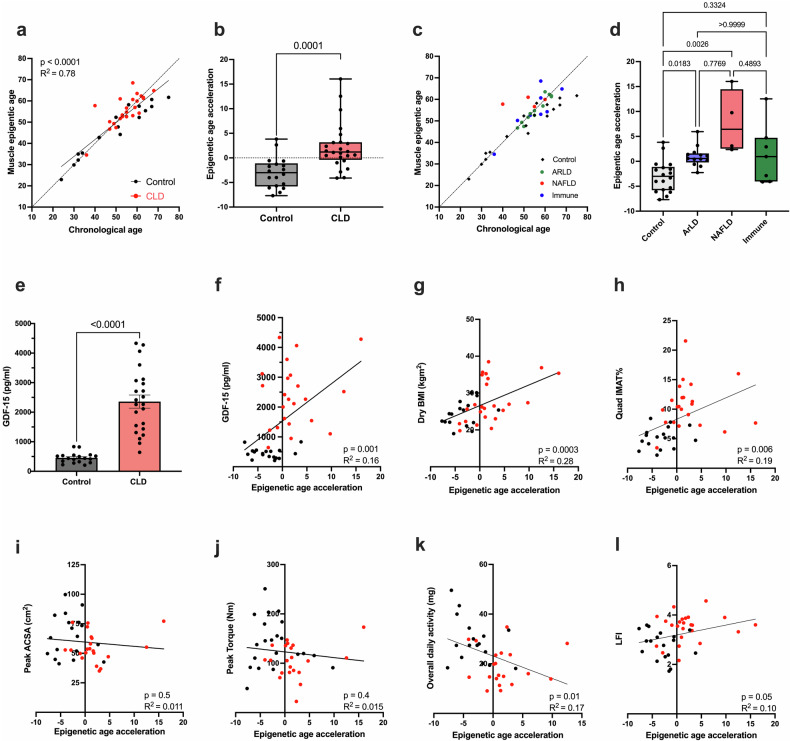
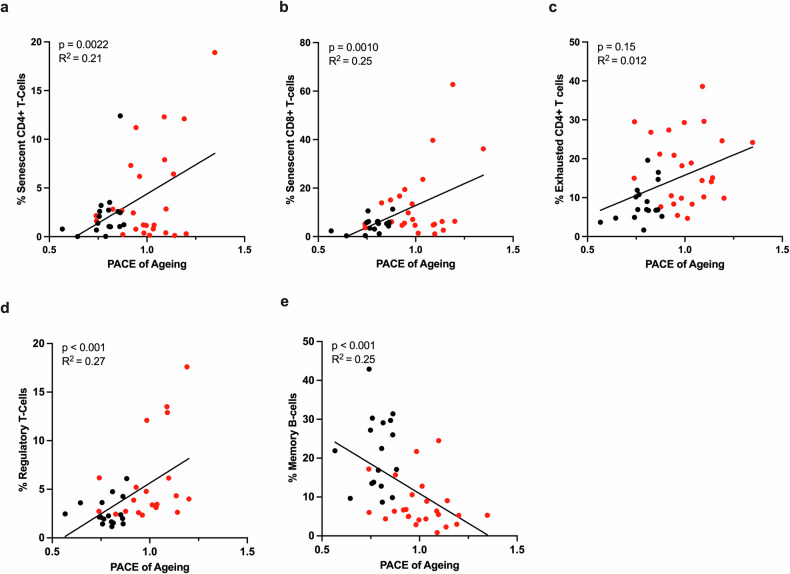
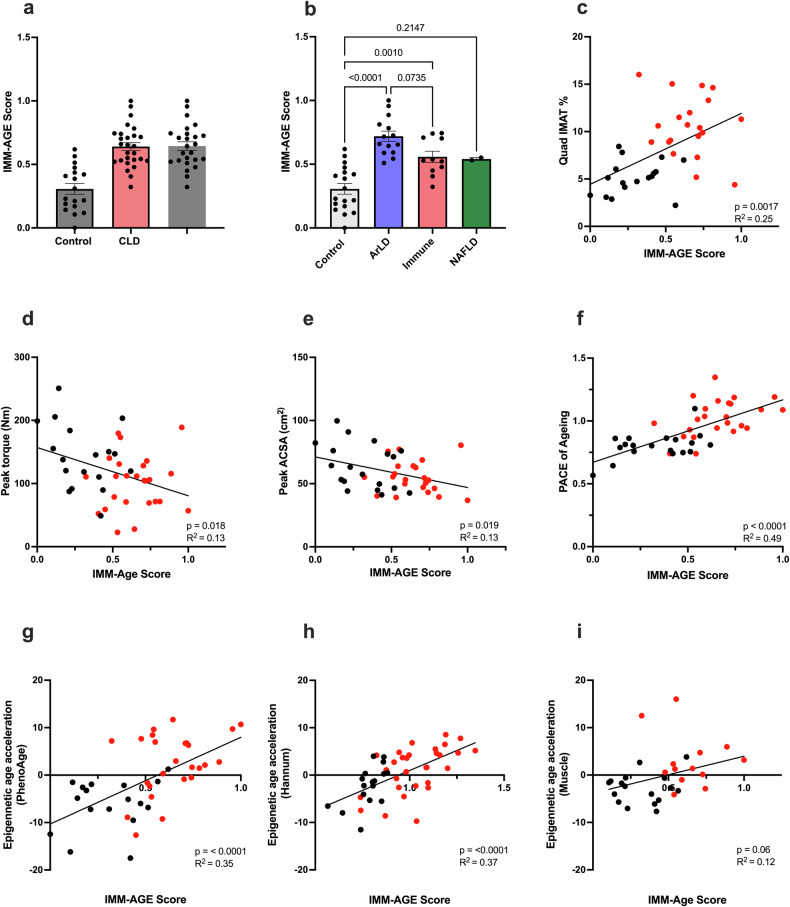
Patients with chronic liver disease (CLD) often present with significant frailty, sarcopenia, and impaired immune function. However, the mechanisms driving the development of these age-related phenotypes are not fully understood. To determine whether accelerated biological aging may play a role in CLD, epigenetic, transcriptomic, and phenotypic assessments were performed on the skeletal muscle tissue and immune cells of CLD patients and age-matched healthy controls. Accelerated biological aging of the skeletal muscle tissue of CLD patients was detected, as evidenced by an increase in epigenetic age compared with chronological age (mean +2.2 ± 4.8 years compared with healthy controls at -3.0 ± 3.2 years, p = 0.0001). Considering disease etiology, age acceleration was significantly greater in both the alcohol-related (ArLD) (p = 0.01) and nonalcoholic fatty liver disease (NAFLD) (p = 0.0026) subgroups than in the healthy control subgroup, with no age acceleration observed in the immune-mediated subgroup or healthy control subgroup (p = 0.3). The skeletal muscle transcriptome was also enriched for genes associated with cellular senescence. Similarly, blood cell epigenetic age was significantly greater than that in control individuals, as calculated using the PhenoAge (p < 0.0001), DunedinPACE (p < 0.0001), or Hannum (p = 0.01) epigenetic clocks, with no difference using the Horvath clock. Analysis of the IMM-Age score indicated a prematurely aged immune phenotype in CLD patients that was 2-fold greater than that observed in age-matched healthy controls (p < 0.0001). These findings suggested that accelerated cellular aging may contribute to a phenotype associated with advanced age in CLD patients. Therefore, therapeutic interventions to reduce biological aging in CLD patients may improve health outcomes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
