

Interactions between patterns of multimorbidity and functional status among hospitalized older patients: a novel approach using cluster analysis and association rule mining
- PMID: 39026203
- PMCID: PMC11264579
- DOI: 10.1186/s12967-024-05444-9
Interactions between patterns of multimorbidity and functional status among hospitalized older patients: a novel approach using cluster analysis and association rule mining
Abstract
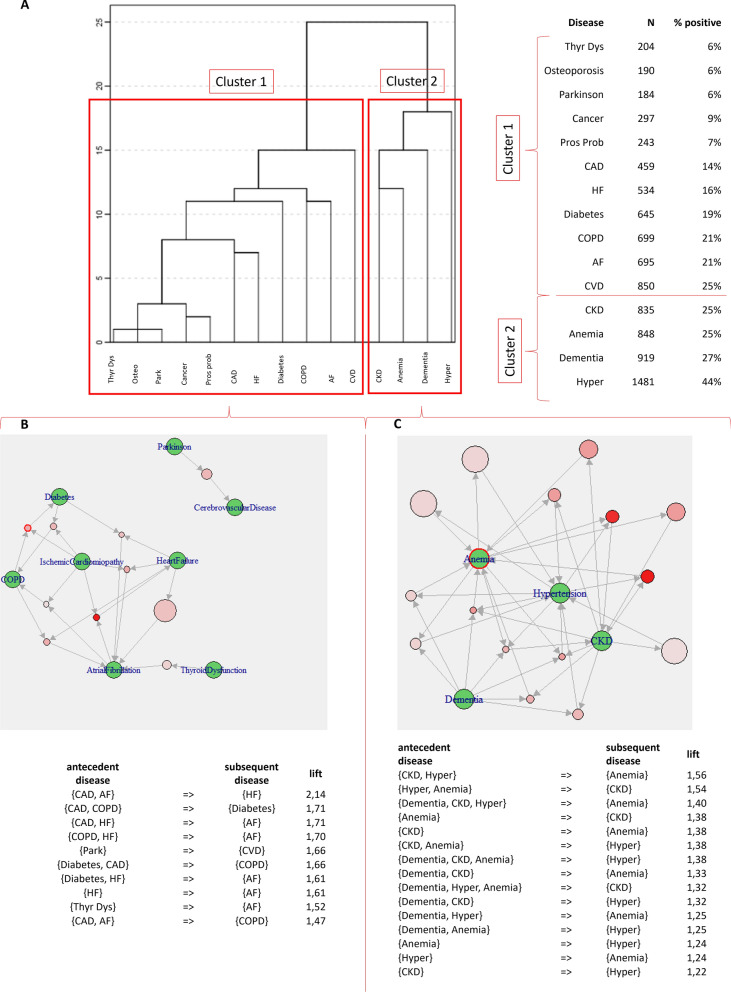
Background: Multimorbidity (MM) is generally defined as the presence of 2 or more chronic diseases in the same patient and seems to be frequently associated with frailty and poor quality of life. However, the complex interplay between MM and functional status in hospitalized older patients has not been fully elucidated so far. Here, we implemented a 2-step approach, combining cluster analysis and association rule mining to explore how patterns of MM and disease associations change as a function of disability.
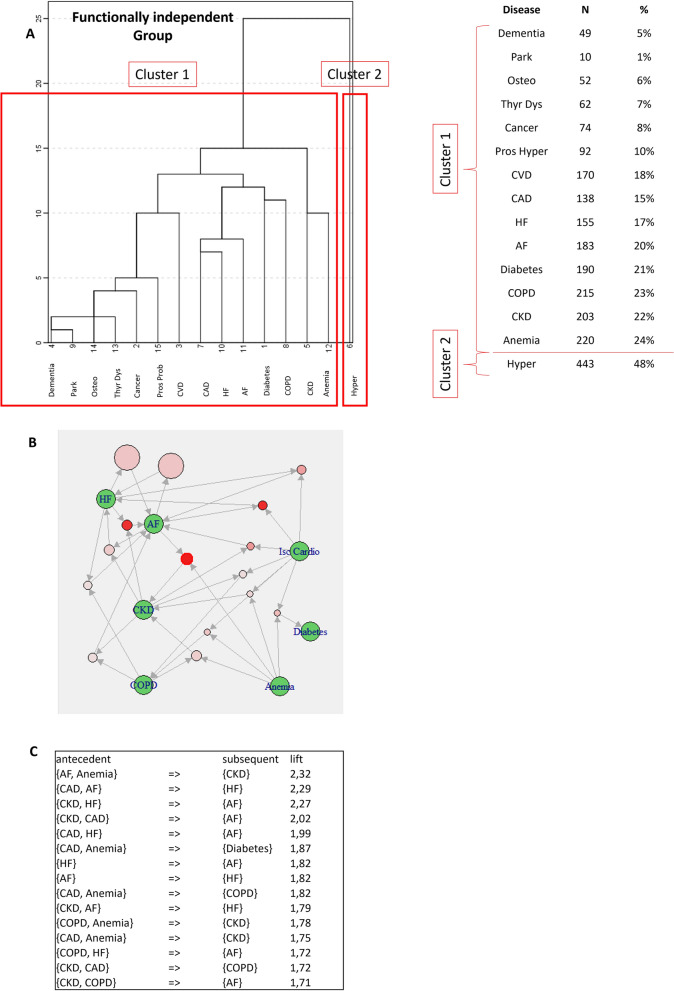
Methods: This retrospective cohort study included 3366 hospitalized older patients discharged from acute care units of Ancona and Cosenza sites of Italian National Institute on Aging (INRCA-IRCCS) between 2011 and 2017. Cluster analysis and association rule mining (ARM) were used to explore patterns of MM and disease associations in the whole population and after stratifying by dependency in activities of daily living (ADL) at discharge. Sensitivity analyses in men and women were conducted to test for robustness of study findings.
Results: Out of 3366 included patients, 78% were multimorbid. According to functional status, 22.2% of patients had no disability in ADL (functionally independent group), 22.7% had 1 ADL dependency (mildly dependent group), and 57.4% 2 or more ADL impaired (moderately-severely dependent group). Two main MM clusters were identified in the whole general population and in single ADL groups. ARM revealed interesting within-cluster disease associations, characterized by high lift and confidence. Specifically, in the functionally independent group, the most significant ones involved atrial fibrillation (AF)-anemia and chronic kidney disease (CKD) (lift = 2.32), followed by coronary artery disease (CAD)-AF and heart failure (HF) (lift = 2.29); in patients with moderate-severe ADL disability, the most significant ARM involved CAD-HF and AF (lift = 1.97), thyroid dysfunction and AF (lift = 1.75), cerebrovascular disease (CVD)-CAD and AF (lift = 1.55), and hypertension-anemia and CKD (lift = 1.43).
Conclusions: Hospitalized older patients have high rates of MM and functional impairment. Combining cluster analysis to ARM may assist physicians in discovering unexpected disease associations in patients with different ADL status. This could be relevant in the view of individuating personalized diagnostic and therapeutic approaches, according to the modern principles of precision medicine.
Keywords: Association rule mining; Cluster analysis; Functional status; Hospitalization; Multimorbidity; Older patients.
© 2024. The Author(s).
Conflict of interest statement
All Authors declare to have no conflict of interest with the content of this manuscript.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
