

Bronchiectasis
- PMID: 39026515
- PMCID: PMC11255363
- DOI: 10.1016/j.opresp.2024.100339
Bronchiectasis
Abstract
Non-cystic fibrosis bronchiectasis, a condition that remains relatively underrecognized, has garnered increasing research focus in recent years. This scientific interest has catalyzed advancements in diagnostic methodologies, enabling comprehensive clinical and molecular profiling. Such progress facilitates the development of personalized treatment strategies, marking a significant step toward precision medicine for these patients. Bronchiectasis poses significant diagnostic challenges in both clinical settings and research studies. While computed tomography (CT) remains the gold standard for diagnosis, novel alternatives are emerging. These include artificial intelligence-powered algorithms, ultra-low dose chest CT, and magnetic resonance imaging (MRI) techniques, all of which are becoming recognized as feasible diagnostic tools. The precision medicine paradigm calls for refined characterization of bronchiectasis patients by analyzing their inflammatory and molecular profiles. Research into the underlying mechanisms of inflammation and the evaluation of biomarkers such as neutrophil elastase, mucins, and antimicrobial peptides have led to the identification of distinct patient endotypes. These endotypes present variable clinical outcomes, necessitating tailored therapeutic interventions. Among these, eosinophilic bronchiectasis is notable for its prevalence and specific prognostic factors, calling for careful consideration of treatable traits. A deeper understanding of the microbiome's influence on the pathogenesis and progression of bronchiectasis has inspired a holistic approach, which considers the multibiome as an interconnected microbial network rather than treating pathogens as solitary entities. Interactome analysis therefore becomes a vital tool for pinpointing alterations during both stable phases and exacerbations. This array of innovative approaches has revolutionized the personalization of treatments, incorporating therapies such as inhaled mannitol or ARINA-1, brensocatib for anti-inflammatory purposes, and inhaled corticosteroids specifically for patients with eosinophilic bronchiectasis.
Las bronquiectasias no fibrosis quística han atraído una creciente atención en investigación. Este interés científico ha catalizado avances en las metodologías de diagnóstico, permitiendo realizar perfiles clínicos y moleculares integrales. Este progreso facilita el desarrollo de estrategias de tratamiento personalizadas y marca un paso significativo hacia la medicina de precisión.Desde el punto de vista diagnóstico, las bronquiectasias plantean desafíos importantes en entornos clínicos y de investigación. Si bien la TC es el gold standard, están surgiendo nuevas alternativas. Entre ellas, algoritmos de inteligencia artificial, TC de tórax de dosis ultrabajas y técnicas de resonancia magnética.La medicina de precisión aboga por la caracterización de pacientes mediante análisis de perfiles inflamatorios y moleculares. Las investigaciones sobre mecanismos subyacentes de inflamación y la evaluación de biomarcadores como la elastasa de neutrófilos, mucinas y péptidos antimicrobianos, han llevado a la identificación de endotipos de pacientes. Estos endotipos exhiben resultados clínicos variables, requiriendo intervenciones terapéuticas personalizadas. La bronquiectasia eosinofílica destaca por su prevalencia y factores pronósticos específicos, exigiendo consideración de los rasgos tratables.Una comprensión profunda de la influencia del microbioma en la patogénesis y progresión de las bronquiectasias inspira un enfoque holístico. Considera el multibioma como una red microbiana interconectada, no entidades solitarias. El análisis del interactoma se convierte en una herramienta vital para identificar alteraciones durante fases estables y exacerbaciones.Este conjunto de enfoques innovadores revoluciona la personalización de los tratamientos, incorporando terapias como manitol inhalado o ARINA-1, brensocatib con fines antiinflamatorios y corticosteroides inhalados específicos para pacientes con bronquiectasias eosinofílicas.
Keywords: Bronchiectasis; Bronchiectasis endotypes; Lung microbiome.
© 2024 Sociedad Española de Neumología y Cirugía Torácica (SEPAR). Published by Elsevier España, S.L.U.
Figures
References
-
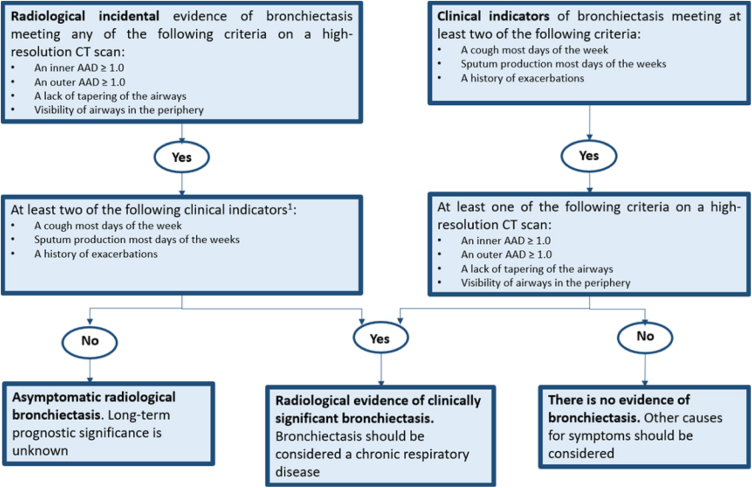
- Aliberti S., Goeminne P.C., O’Donnell A.E., Aksamit T.R., Al-Jahdali H., Barker A.F., et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: international consensus recommendations. Lancet Respir Med. 2022;10:298–306. doi: 10.1016/S2213-2600(21)00277-0. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
