

Influence of sarcopenia on postoperative complications and long-term survival in pancreatic cancer patients undergone pancreaticoduodenectomy
- PMID: 39027658
- PMCID: PMC11254807
- DOI: 10.3389/fnut.2024.1434630
Influence of sarcopenia on postoperative complications and long-term survival in pancreatic cancer patients undergone pancreaticoduodenectomy
Abstract
Background: Sarcopenia has the potential to impact the postoperative results and extended prognosis of various types of tumors. Nevertheless, the specific impact of sarcopenia on the postoperative results and long-term survival of pancreatic cancer (PC) following pancreaticoduodenectomy (PD) remains inadequately elucidated. This study investigates the significance of sarcopenia according to various Asian standards on postoperative complications and long-term prognosis in PC patients who have undergone PD.
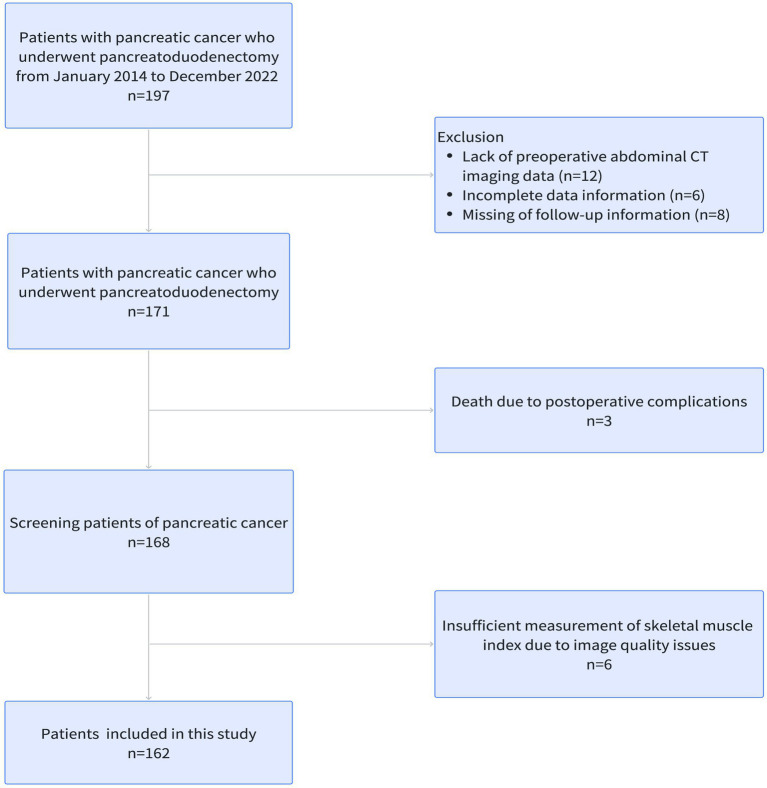
Methods: This retrospective study systematically analyzed patients with PC who underwent PD from January 2015 to December 2022. Sarcopenia was diagnosed by the skeletal muscle index (SMI) obtained by the skeletal muscle area normalized for height squared on the third lumbar vertebra on computed tomography (CT) images. Univariate and multivariate logistic regression analysis were performed to analyze the correlation between sarcopenia and postoperative complications, while Cox regression analysis was utilized to explore the influence of sarcopenia on overall survival (OS) and recurrence-free survival (RFS) in PC patients after PD.
Results: We enrolled 162 patients with PC after PD (92 males and 70 females, mean age: 63.78 ± 10.27 years), including 83 and 79 patients with sarcopenia and non-sarcopenia, respectively. Compared with non-sarcopenia patients, sarcopenia exhibited higher rates of recurrence rate (75% versus 59%, p = 0.039). Univariate and multivariate logistic regression analysis showed that sarcopenia did not affect the incidence of complications in patients with PC after PD in three Asian sarcopenia criteria. Multivariate Cox regression analysis indicated that sarcopenia was an independent risk factor for OS (hazard ratio [HR]: 2.49, 95% confidence interval [CI]: 1.73-3.60, p < 0.001) and RFS(hazard ratio [HR]: 1.70, 95%confidence interval [CI]: 1.12-2.50, p = 0.012) of PC patients with PD in Japanese Society of Hepatology criteria. Meanwhile, according to the Asian pancreatic cancer population standard, sarcopenia is an independent risk factor affecting the long-term OS (hazard ratio [HR]: 2.59, 95% confidence interval [CI]: 1.80-3.70, p < 0.001) and RFS (hazard ratio [HR]: 2.00, 95% confidence interval [CI]: 1.36-3.00, p < 0.001) of PC after PD. While sarcopenia is recognized as a risk factor for OS (hazard ratio [HR]: 1.81, 95% confidence interval [CI]: 1.08-3.10, p = 0.025) in PC patients based on the Fujiwara criteria, it is not found to be associated with RFS (hazard ratio [HR]: 1.60, 95% confidence interval [CI]: 0.90-3.00, p = 0.10). The model based on sarcopenia and clinical characteristics has high predictive ability for OS and RFS.
Conclusion: Various Asian diagnostic criteria do not link sarcopenia with postoperative complications in PC patients after PD. Nevertheless, sarcopenia remains a significant independent risk factor for long-term survival, and its combination with clinical characteristics can aid clinicians in predicting long-term survival outcomes.
Keywords: complications; pancreatic cancer; pancreaticoduodenectomy; sarcopenia; skeletal muscle index.
Copyright © 2024 Qu, Zhou, Zhang, Lyu and Lang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Slidell MB, Chang DC, Cameron JL, Wolfgang C, Herman JM, Schulick RD, et al. . Impact of total lymph node count and lymph node ratio on staging and survival after pancreatectomy for pancreatic adenocarcinoma: a large, population-based analysis. Ann Surg Oncol. (2008) 15:165–74. doi: 10.1245/s10434-007-9587-1, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources