

Purulent Streptococcus intermedius Pericarditis in the Setting of Histoplasma Mediastinal Lymphadenitis: A Case Report and Literature Review
- PMID: 39027746
- PMCID: PMC11257658
- DOI: 10.7759/cureus.62626
Purulent Streptococcus intermedius Pericarditis in the Setting of Histoplasma Mediastinal Lymphadenitis: A Case Report and Literature Review
Abstract
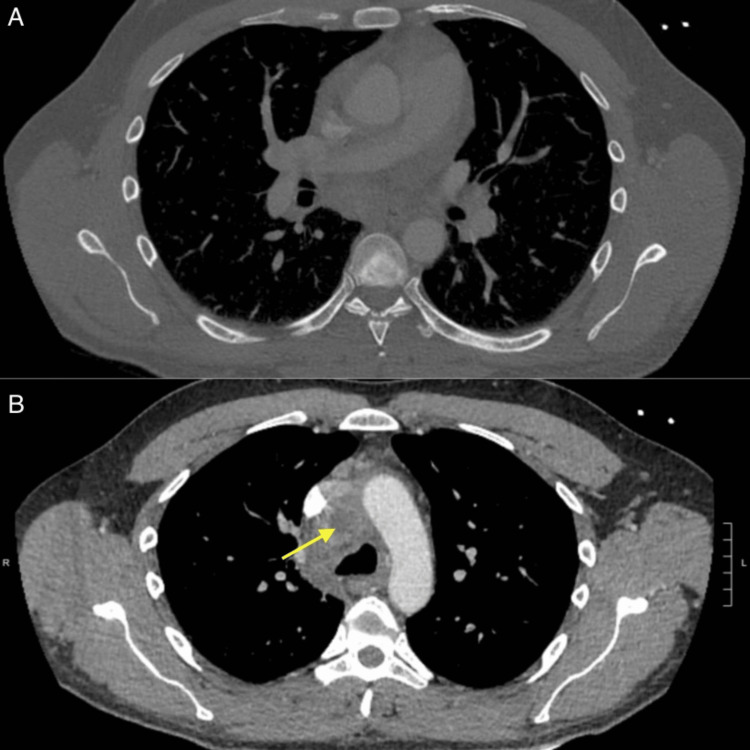
Purulent pericarditis is a rare and potentially life-threatening condition characterized by infection of the pericardial space. We describe a case of purulent bacterial pericarditis in a 41-year-old male with no significant medical or surgical history who had concomitant pulmonary Histoplasma infection. Streptococcus intermedius was the bacteria directly responsible for the pericardial infection, though co-infection with histoplasmosis likely predisposed him to develop purulent pericarditis. We hypothesize histoplasmosis caused mediastinal lymphadenopathy, facilitating contact between a necrotic lymph node and the pericardium and contiguous suppuration of bacteria to the pericardial space. We treated S. intermedius and Histoplasma capsulatum with ceftriaxone and amphotericin B, respectively. Additionally, the patient presented in cardiac tamponade requiring emergent pericardiocentesis and drain placement. His course was also complicated by pericardial constriction. Cardiac magnetic resonance confirmed this, showing inflamed pericardium and abnormal septal motion with inspiration, and he had symptoms refractory to antimicrobials and anti-inflammatories. As such, he required pericardiectomy. This case demonstrates maintaining suspicion for secondary infectious foci as a contributor to the pathogenesis of purulent pericarditis is important, as pulmonary histoplasmosis played a pivotal role in allowing S. intermedius to spread to the pericardium but was not the primary infection. It also highlights the multifaceted evaluation and management of purulent pericarditis, highlighting the role of echocardiography and emergent pericardial drainage if cardiac tamponade is present, the importance of targeted antimicrobial therapy, the superior ability of cardiac magnetic resonance to identify pericardial constriction as a sequela of purulent pericarditis, and indications for pericardiectomy.
Keywords: constrictive pericarditis; histoplasma in immunocompetent patient; pericardiectomy; purulent pericarditis; tamponade physiology.
Copyright © 2024, Christian-Miller et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures






References
-
- Purulent pericarditis: review of a 20-year experience in a general hospital. Sagristà-Sauleda J, Barrabés JA, Permanyer-Miralda G, Soler-Soler J. J Am Coll Cardiol. 1993;22:1661–1665. - PubMed
-
- The changed spectrum of purulent pericarditis: an 86 year autopsy experience in 200 patients. Klacsmann PG, Bulkley BH, Hutchins GM. Am J Med. 1977;63:666–673. - PubMed
-
- 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: the Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS) Adler Y, Charron P, Imazio M, et al. Eur Heart J. 2015;36:2921–2964. - PMC - PubMed
-
- Cardiac magnetic resonance imaging of pericardial diseases: a comprehensive guide. Antonopoulos AS, Vrettos A, Androulakis E, et al. Eur Heart J Cardiovasc Imaging. 2023;24:983–998. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials