

Feeling a Little Blue After Ablation: Iatrogenic Atrial Septal Defect With Right-to-Left Shunt Following Atrial Fibrillation Ablation
- PMID: 39027752
- PMCID: PMC11257765
- DOI: 10.7759/cureus.62629
Feeling a Little Blue After Ablation: Iatrogenic Atrial Septal Defect With Right-to-Left Shunt Following Atrial Fibrillation Ablation
Abstract
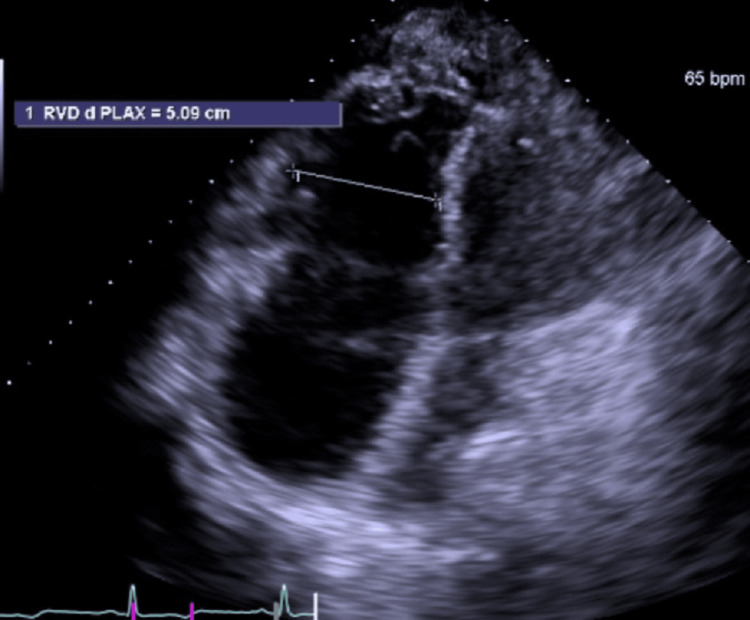
Atrial fibrillation is the most common cardiac arrhythmia. Cardiac ablation is indicated for patients refractory to medical management. During the ablation process, a transseptal puncture is utilized to access and isolate the pulmonary veins, which results in a temporary iatrogenic atrial septal defect (iASD). Generation of an iASD is considered unavoidable and is a generally accepted risk due to high rates of spontaneous closure. Studies have shown that persisting iASD may occur in 5%-20% of patients for up to nine to 12 months after undergoing radiofrequency ablation and that spontaneous rates of closure are high in patients with normal intracardiac pressures. Patients with preexisting elevated right intracardiac pressures from pulmonary hypertension or other right-sided cardiac pathology are at an increased risk of complications from iASD. These increased pressures can lead to clinically significant hypoxemia from right-to-left shunting following a transseptal puncture. Intervention with closure is considered in high-risk settings such as right atrial or ventricular enlargement, right-to-left shunting with hypoxemia, and intraseptal defect greater than 8 mm. This case vignette describes a 67-year-old female who developed clinically significant right-to-left shunting intraoperatively from iASD with ongoing hypoxemia for several months but with spontaneous closure. We highlight this case as it demonstrates spontaneous closure in a high-risk iASD. We also provide a review of the literature on iASD after cardiac ablations.
Keywords: atrial fibrillation; atrial septal defect; cryotherapy and laser cardiac ablation; iatrogenic atrial septal defect; intracardiac shunting.
Copyright © 2024, Nguyen et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Community Memorial Hospital Institutional Review Board (IRB) issued approval 2023-CR304. IRB exempt. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Atrial fibrillation: are there gender differences? Michelena HI, Ezekowitz MD. https://pubmed.ncbi.nlm.nih.gov/11253382/ J Gend Specif Med. 2000;3:44–49. - PubMed
-
- Atrial fibrillation pathophysiology: implications for management. Iwasaki YK, Nishida K, Kato T, Nattel S. https://doi.org/10.1161/CIRCULATIONAHA.111.019893. Circulation. 2011;124:2264–2274. - PubMed
-
- Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the cabana randomized clinical trial. Packer DL, Mark DB, Robb RA, et al. http://.PMID: 30874766 PMCID: PMC6450284. JAMA. 2019;321:1261–1274. - PMC - PubMed
-
- Ablation of atrial fibrillation: patient selection, periprocedural anticoagulation, techniques, and preventive measures after ablation. Link MS, Haïssaguerre M, Natale A. Circulation. 2016;134:339–352. - PubMed
Publication types
LinkOut - more resources
Full Text Sources