

Battle of the Blocks: Which Pain Management Technique Triumphs in Gender-Affirming Bilateral Mastectomies?
- PMID: 39027810
- PMCID: PMC11254309
- DOI: 10.14740/jocmr5159
Battle of the Blocks: Which Pain Management Technique Triumphs in Gender-Affirming Bilateral Mastectomies?
Abstract
Background: Gender-affirming mastectomy, performed on transgender men and non-binary individuals, frequently leads to considerable postoperative pain. This pain can significantly affect both patient satisfaction and the overall recovery process. The study examines the efficacy of four analgesic techniques pectoral nerve (PECS) 2 block, erector spinae plane (ESP) block, thoracic wall local anesthesia infiltration (TWI), and systemic multimodal analgesia (SMA) in managing perioperative pain, with special consideration for the effects of chronic testosterone therapy on pain thresholds.
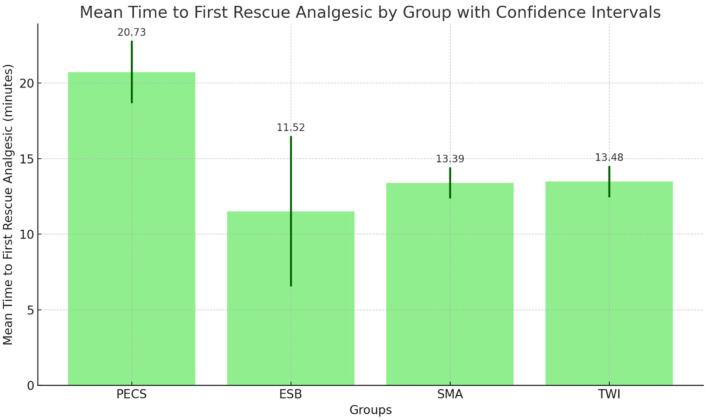
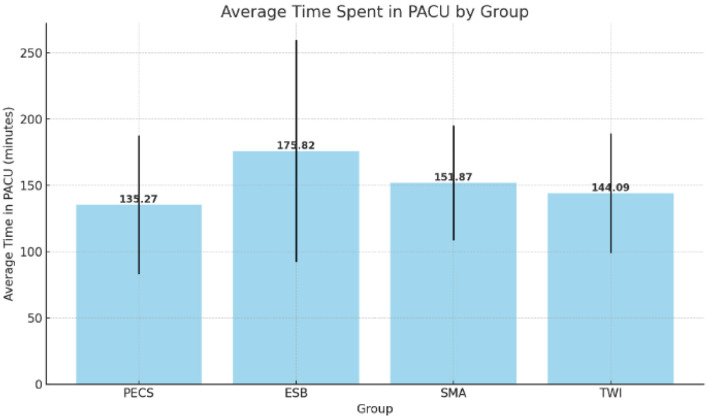
Methods: A retrospective analysis was conducted on patients aged 18 - 45 who underwent gender-affirming bilateral mastectomies at a New York City community hospital. The study compared intraoperative and post-anesthesia care unit (PACU) opioid consumption, postoperative pain scores, the interval to first rescue analgesia, and total PACU duration among the four analgesic techniques.
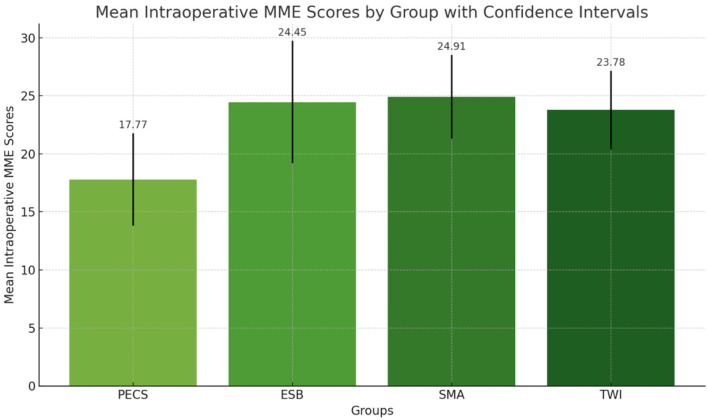
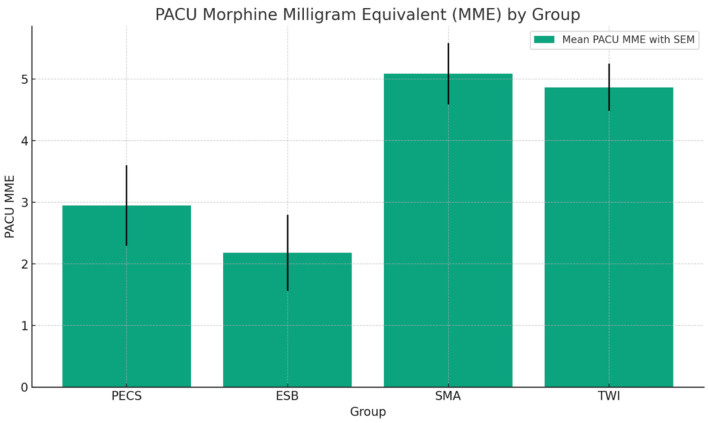
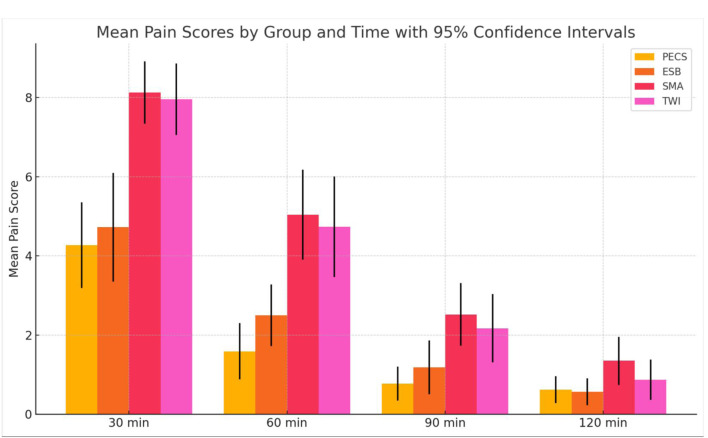
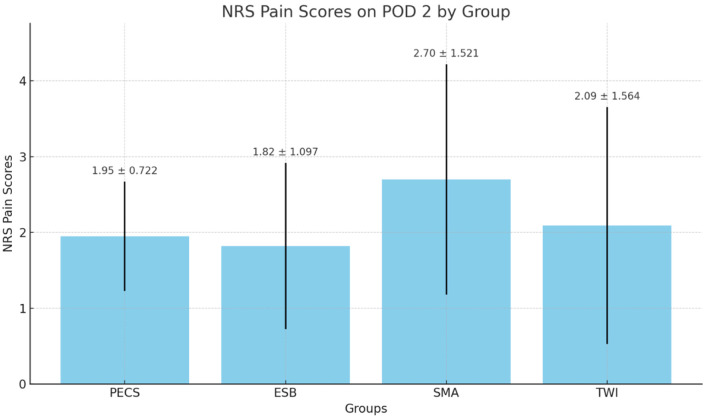
Results: The study found significant differences in intraoperative and PACU opioid consumption across the groups, with the PECS 2 block group showing the least opioid requirement. The PACU morphine milligram equivalent (MME) consumption was highest in the SMA group. Postoperative pain scores were significantly lower in the PECS and ESP groups at earlier time points post-surgery. However, by postoperative day 2, pain scores did not significantly differ among the groups. Chronic testosterone therapy did not significantly impact intraoperative opioid requirements.
Conclusion: The PECS 2 block is superior in reducing overall opioid consumption and providing effective postoperative pain control in gender-affirming mastectomies. The study underscores the importance of tailoring pain management strategies to the unique physiological responses of the transgender and non-binary community. Future research should focus on prospective designs, standardized block techniques, and the complex relationship between hormonal therapy and pain perception.
Keywords: Analgesic efficacy; Chronic testosterone therapy; Erector spinae plane block; Gender-affirming mastectomy; Non-binary individuals; Pectoral nerve block; Retrospective analysis; Thoracic wall infiltration.
Copyright 2024, Sivakumar et al.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Alcon A, Kennedy A, Wang E, Piper M, Loeliger K, Admassu N, Lentz R. et al. Quantifying the psychosocial benefits of masculinizing mastectomy in trans male patients with patient-reported outcomes: the University of California, San Francisco, gender quality of life survey. Plast Reconstr Surg. 2021;147(5):731e–740e. doi: 10.1097/PRS.0000000000007883. - DOI - PubMed
-
- Rokhtabnak F, Sayad S, Izadi M, Djalali Motlagh S, Rahimzadeh P. Pain control after mastectomy in transgender patients: ultrasound-guided pectoral nerve block II versus conventional intercostal nerve block: a randomized clinical trial. Anesth Pain Med. 2021;11(5):e119440. doi: 10.5812/aapm.119440. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous