

Left atrial appendage closure for stroke prevention in atrial fibrillation: current status and perspectives
- PMID: 39027946
- PMCID: PMC11335376
- DOI: 10.1093/eurheartj/ehae398
Left atrial appendage closure for stroke prevention in atrial fibrillation: current status and perspectives
Abstract
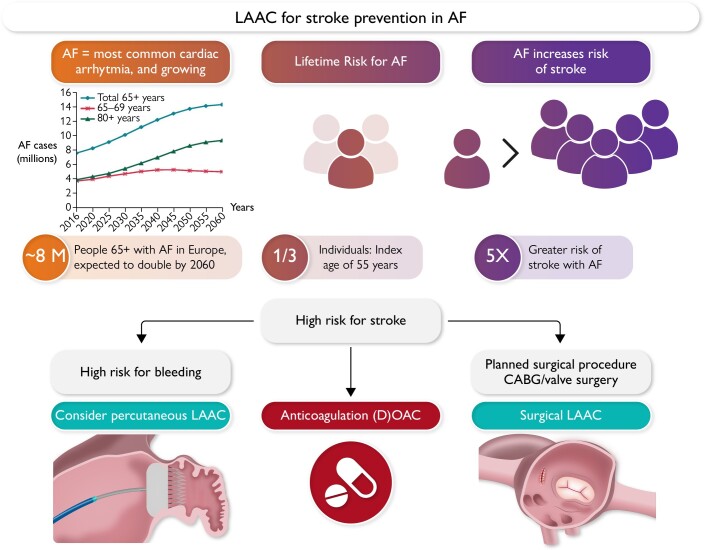
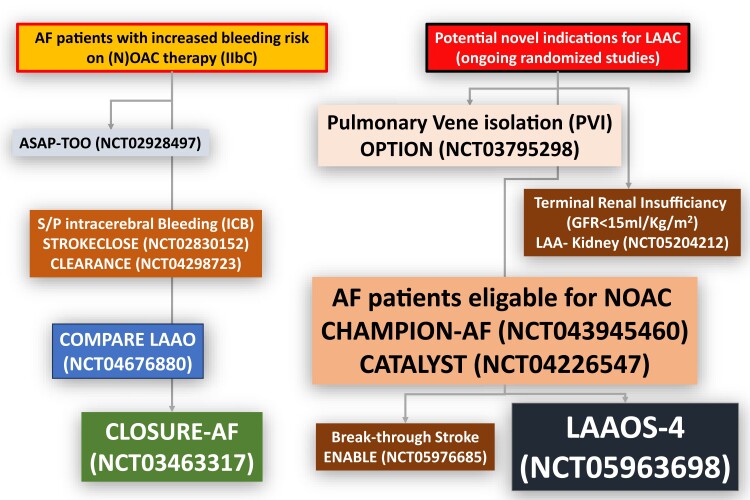
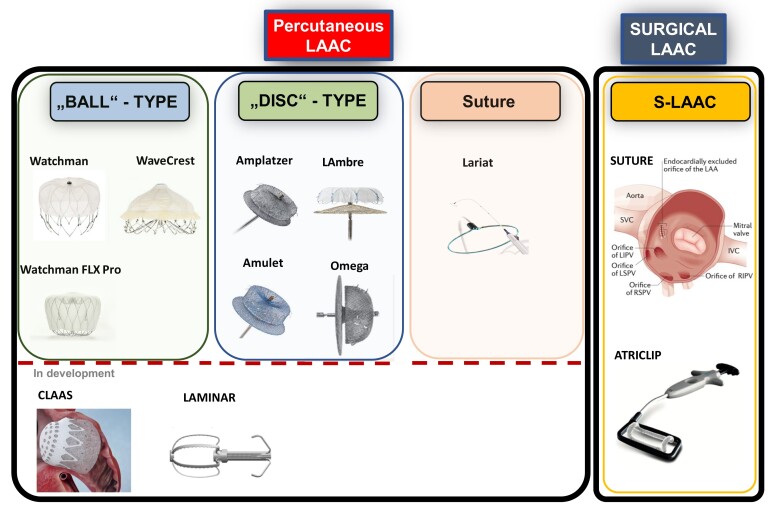
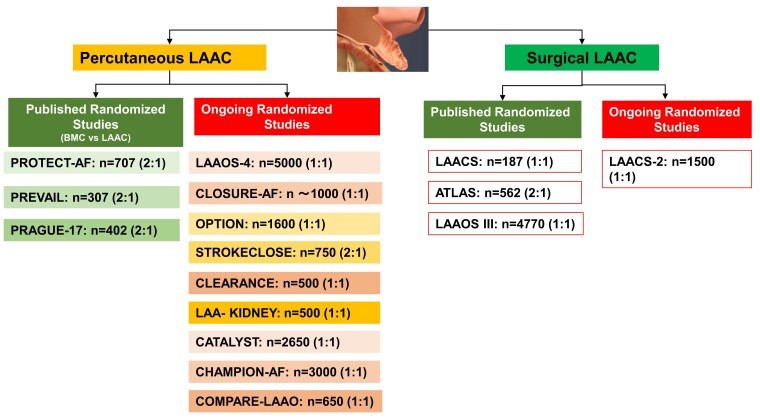
Atrial fibrillation (AF) is associated with an increased risk of stroke and systemic embolism, and the left atrial appendage (LAA) has been identified as a principal source of thromboembolism in these patients. While oral anticoagulation is the current standard of care, LAA closure (LAAC) emerges as an alternative or complementary treatment approach to reduce the risk of stroke or systemic embolism in patients with AF. Moderate-sized randomized clinical studies have provided data for the efficacy and safety of catheter-based LAAC, largely compared with vitamin K antagonists. LAA device iterations, advances in pre- and peri-procedural imaging, and implantation techniques continue to increase the efficacy and safety of LAAC. More data about efficacy and safety of LAAC have been collected, and several randomized clinical trials are currently underway to compare LAAC with best medical care (including non-vitamin K antagonist oral anticoagulants) in different clinical settings. Surgical LAAC in patients with AF undergoing cardiac surgery reduced the risk of stroke on background of anticoagulation therapy in the LAAOS III study. In this review, we describe the rapidly evolving field of LAAC and discuss recent clinical data, ongoing studies, open questions, and current limitations of LAAC.
Keywords: Atrial fibrillation; Left atrial appendage closure; Oral anticoagulation; Stroke prevention.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. . 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373–498. 10.1093/eurheartj/ehaa612 - DOI - PubMed
-
- Lamassa M, Di Carlo A, Pracucci G, Basile AM, Trefoloni G, Vanni P, et al. . Characteristics, outcome, and care of stroke associated with atrial fibrillation in Europe: data from a multicenter multinational hospital-based registry (the European Community Stroke Project). Stroke 2001;32:392–8. 10.1161/01.STR.32.2.392 - DOI - PubMed
