

Fluoroscopy-Guided Percutaneous Transthoracic Pleural Forceps Biopsy in Patients With Exudative Pleural Effusion
- PMID: 39028012
- PMCID: PMC11306004
- DOI: 10.3348/kjr.2023.0960
Fluoroscopy-Guided Percutaneous Transthoracic Pleural Forceps Biopsy in Patients With Exudative Pleural Effusion
Abstract
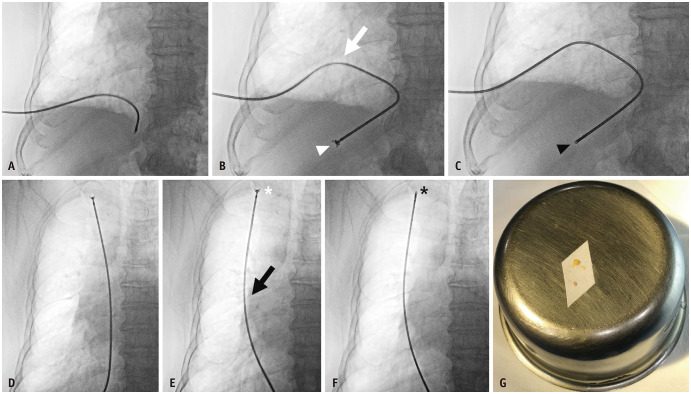
Objective: This study aimed to evaluate the diagnostic performance and procedural characteristics of fluoroscopy-guided percutaneous transthoracic pleural forceps biopsy (PTPFB) in patients with exudative pleural effusion.
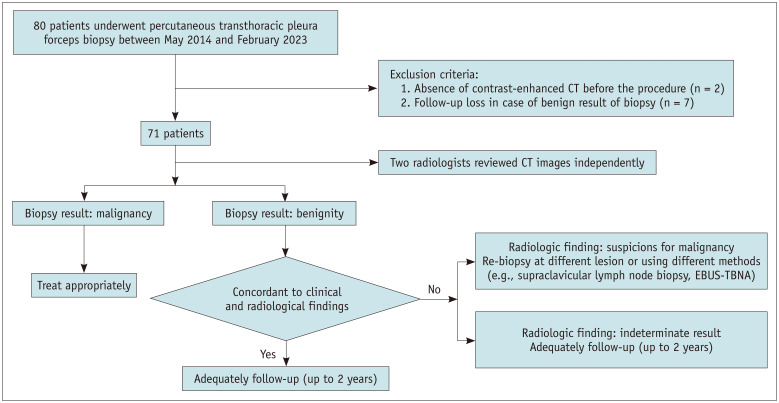
Materials and methods: Patients with exudative pleural effusion who underwent PTPFB between May 1, 2014, and February 28, 2023, were included in this retrospective study. The interval between percutaneous catheter drainage (PCD) and PTPFB, number of biopsies, procedural time, and procedure-related complications were evaluated. The sensitivity, specificity, and accuracy of diagnosing malignancy were computed for pleural cytology using PCD drainage, PTPFB, and combined PTPFB and pleural cytology.
Results: Seventy-one patients, comprising 50 male and 21 female (mean age, 69.5 ± 15.3 years), were included in this study. The final diagnoses were benign lesions in 48 patients (67.6%) and malignant in 23 patients (32.4%). The overall interval between PCD and biopsy was 2.4 ± 3.7 days. The interval between PCD and biopsy in the group that underwent delayed PTPFB was 5.2 ± 3.9 days. The mean number of biopsies was 4.5 ± 1.3. The mean procedural time was 4.4 ± 2.1 minutes. Minor bleeding complications were reported in one patient (1.4%). The sensitivity, specificity, and accuracy for pleural cytology, PTPFB, and combined PTPFB and pleural cytology were 47.8% (11/23), 100% (48/48), and 83.1% (59/71), respectively; 65.2% (15/23), 100% (48/48), and 88.7% (63/71), respectively; and 78.3% (18/23), 100% (48/48), and 93.0% (66/71), respectively. The sensitivity and accuracy of cytology combined with PTPFB were significantly higher than those of cytological testing alone (P = 0.008 and 0.001, respectively).
Conclusion: Fluoroscopy-guided PTPFB is an accurate and safe diagnostic technique for patients with exudative pleural effusion, with acceptable diagnostic performance, low complication rates, and reasonable procedural times.
Keywords: Biopsy; Exudate; Fluoroscopy; Forceps; Percutaneous; Pleura.
Copyright © 2024 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Walker SP, Morley AJ, Stadon L, De Fonseka D, Arnold DT, Medford ARL, et al. Nonmalignant pleural effusions: a prospective study of 356 consecutive unselected patients. Chest. 2017;151:1099–1105. - PubMed
-
- Anevlavis S, Tzouvelekis A, Bouros D. Mechanisms of pleural involvement in orphan diseases. Respiration. 2012;83:5–12. - PubMed
-
- Choi SH, Cha SI, Shin KM, Lim JK, Yoo SS, Lee SY, et al. Clinical relevance of pleural effusion in patients with pulmonary embolism. Respiration. 2017;93:271–278. - PubMed
-
- Bintcliffe OJ, Hooper CE, Rider IJ, Finn RS, Morley AJ, Zahan-Evans N, et al. Unilateral pleural effusions with more than one apparent etiology. A prospective observational study. Ann Am Thorac Soc. 2016;13:1050–1056. - PubMed
-
- Evans AL, Gleeson FV. Radiology in pleural disease: state of the art. Respirology. 2004;9:300–312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
