

Safety and Efficacy of SAB-185 for Nonhospitalized Adults With COVID-19: A Randomized Clinical Trial
- PMID: 39028902
- PMCID: PMC11566225
- DOI: 10.1093/infdis/jiae369
Safety and Efficacy of SAB-185 for Nonhospitalized Adults With COVID-19: A Randomized Clinical Trial
Abstract
Background: We evaluated the fully human polyclonal antibody product SAB-185 in a phase 3 trial for COVID-19.
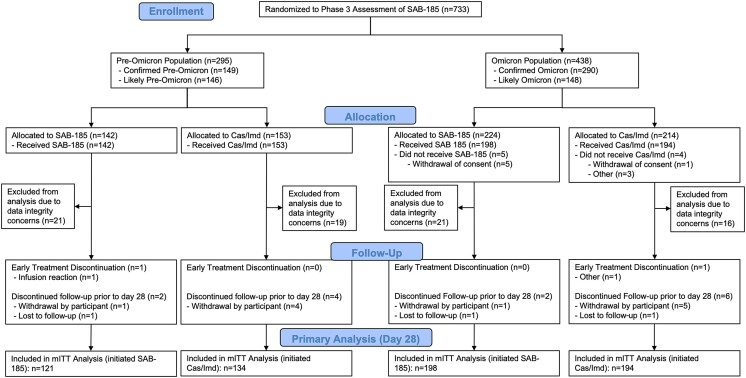
Methods: Nonhospitalized high-risk adults within 7 days of symptom onset were randomized 1:1 to open-label SAB-185 3840 units/kg or casirivimab/imdevimab 1200 mg. Noninferiority comparison was undertaken for pre-Omicron population (casirivimab/imdevimab expected to be fully active) and superiority comparison for the Omicron population (casirivimab/imdevimab not expected to be active). Primary outcomes were the composite of all-cause hospitalizations/deaths and grade ≥3 treatment-emergent adverse events (TEAEs) through day 28. A secondary outcome was time to sustained symptom resolution.
Results: Enrollment ended early due to low hospitalization/death rates upon Omicron emergence; 255 adults were in pre-Omicron and 392 in Omicron populations. Hospitalizations/deaths occurred in 6 (5.0%) and 3 (2.2%) of pre-Omicron SAB-185 and casirivimab/imdevimab arms (absolute difference 2.7%; 95% confidence interval [CI], -2.3%-8.6%); and 5 (2.5%) versus 3 (1.5%) (absolute difference 1.0%; 95% CI, -2.3%-4.5%) for Omicron. All risk ratios for grade ≥3 TEAEs were not significant. Time to symptom resolution was significantly shorter for SAB-185 for Omicron only: 18 versus >25 days; P =.006.
Conclusions: SAB-185 had an acceptable safety profile with faster symptom resolution in the Omicron population.
Clinical trials registration: NCT04518410.
Keywords: COVID-19; SAB-185; casirivimab/imdevimab; outpatient treatment; transchromosomic.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. K. W. C. has consulted for Pardes Biosciences. B. O. T. has received honoraria for advisory boards and consulting from Gilead Sciences. E. S. D. receives consulting fees from Gilead Sciences, Merck, and GSK/ViiV; and research support through the institution from Gilead Sciences and GSK/ViiV. D. A. W. has received funding to the institution to support research; and honoraria for advisory boards and consulting from Gilead Sciences. J. Z. L. has consulted for Abbvie. W. F. has received research funding to the institution from Ridgeback Biopharmaceuticals; served on adjudication committees for Janssen and Syneos; and consulted for Inhalon Biopharmaceuticals and Merck. A. L. G. reports contract testing from Abbott, Cepheid, Novavax, Pfizer, Janssen, and Hologic; and research support from Gilead and Merck, outside of the described work. J. J. E. is an ad hoc consultant to GSK/VIR; and data monitoring committee chair for Adagio (now Invivyd) phase 3 studies. J. S. C. has consulted for Merck and Company. D. M. S. has consulted for Fluxergy, Kiadis, Linear Therapies, VxBiosciences, Model Medicines, and Bayer Pharmaceuticals. C. B. and T. L. are employees of SAB Biotherapeutics. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

References
-
- World Health Organization . WHO COVID-19 dashboard. https://covid19.who.int/. Accessed 1 May 2023.
-
- Food and Drug Administration . Fact sheet for health care providers. Emergency use authorization (EUA) of bamlanivimab. https://www.fda.gov/media/143603/download. Accessed 3 August 2024.
-
- Food and Drug Administration . Fact sheet for health care providers. Emergency use authorization (EUA) of bamlanivimab and etesevimab. https:///www.fda.gov/media/145802/download. Accessed 3 August 2024.
-
- Food and Drug Administration . Fact sheet for health care providers. Emergency use authorization (EUA) of REGEN-COV (casirivimab and imdevimab). https://www.fda.gov/media/145611/download. Accessed 3 August 2024.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069423/AI/NIAID NIH HHS/United States
- U01 AI069423/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- Regeneron Pharmaceuticals
- National Institute of Allergy and Infectious Diseases
- UM1 AI069432/AI/NIAID NIH HHS/United States
- SAB Biotherapeutics
- UM1AI068636/NH/NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
