

Neoadjuvant Osimertinib for the Treatment of Stage I-IIIA Epidermal Growth Factor Receptor-Mutated Non-Small Cell Lung Cancer: A Phase II Multicenter Study
- PMID: 39028931
- PMCID: PMC11379363
- DOI: 10.1200/JCO.24.00071
Neoadjuvant Osimertinib for the Treatment of Stage I-IIIA Epidermal Growth Factor Receptor-Mutated Non-Small Cell Lung Cancer: A Phase II Multicenter Study
Abstract
Purpose: To assess the safety and efficacy of the third-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor osimertinib as neoadjuvant therapy in patients with surgically resectable stage I-IIIA EGFR-mutated non-small cell lung cancer (NSCLC).
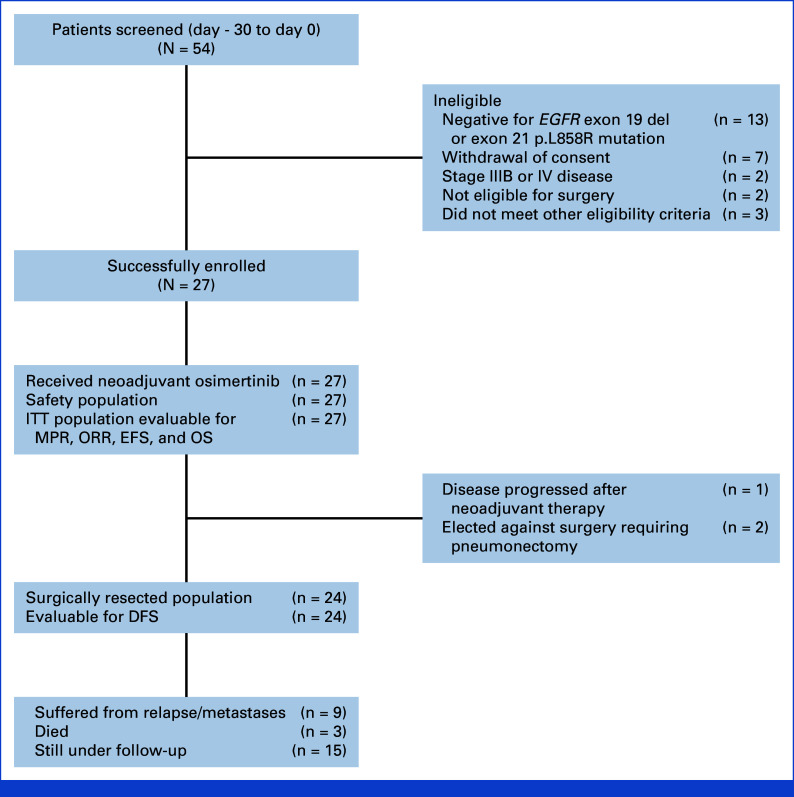
Patients and methods: This was a multi-institutional phase II trial of neoadjuvant osimertinib for patients with surgically resectable stage I-IIIA (American Joint Committee on Cancer [AJCC] V7) EGFR-mutated (L858R or exon 19 deletion) NSCLC (ClinicalTrials.gov identifier: NCT03433469). Patients received osimertinib 80 mg orally once daily for up to two 28-day cycles before surgical resection. The primary end point was major pathological response (MPR) rate. Secondary safety and efficacy end points were also assessed. Exploratory end points included pretreatment and post-treatment tumor mutation profiling.
Results: A total of 27 patients were enrolled and treated with neoadjuvant osimertinib for a median 56 days before surgical resection. Twenty-four (89%) patients underwent subsequent surgery; three (11%) patients were converted to definitive chemoradiotherapy. The MPR rate was 14.8% (95% CI, 4.2 to 33.7). No pathological complete responses were observed. The ORR was 52%, and the median DFS was 40.9 months. One treatment-related serious adverse event (AE) occurred (3.7%). No patients were unable to undergo surgical resection or had surgery delayed because of an AE. The most common co-occurring tumor genomic alterations were in TP53 (42%) and RBM10 (21%).
Conclusion: Treatment with neoadjuvant osimertinib in surgically resectable (stage IA-IIIA, AJCC V7) EGFR-mutated NSCLC did not meet its primary end point for MPR rate. However, neoadjuvant osimertinib did not lead to unanticipated AEs, surgical delays, nor result in a significant unresectability rate.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures






References
-
- Ramalingam SS, Vansteenkiste J, Planchard D, et al. : Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med 382:41-50, 2020 - PubMed
-
- Soria JC, Ohe Y, Vansteenkiste J, et al. : Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med 378:113-125, 2018 - PubMed
-
- Tsuboi M, Herbst RS, John T, et al. : Overall survival with osimertinib in resected EGFR-mutated NSCLC. N Engl J Med 389:137-147, 2023 - PubMed
-
- Blumenthal GM, Bunn PA, Chaft JE, et al. : Current status and future perspectives on neoadjuvant therapy in lung cancer. J Thorac Oncol 13:1818-1831, 2018 - PubMed
-
- Felip E, Rosell R, Maestre JA, et al. : Preoperative chemotherapy plus surgery versus surgery plus adjuvant chemotherapy versus surgery alone in early-stage non-small-cell lung cancer. J Clin Oncol 28:3138-3145, 2010 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
