

A deep learning approach to hard exudates detection and disorganization of retinal inner layers identification on OCT images
- PMID: 39030181
- PMCID: PMC11271624
- DOI: 10.1038/s41598-024-63844-9
A deep learning approach to hard exudates detection and disorganization of retinal inner layers identification on OCT images
Abstract
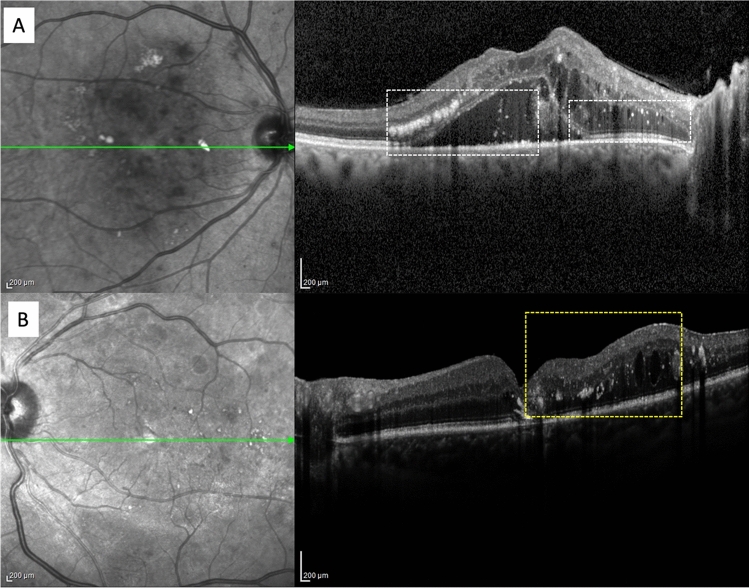
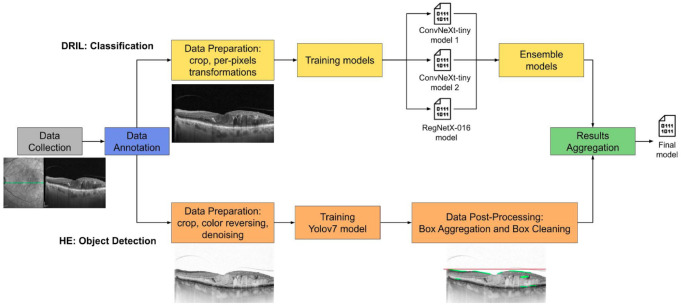
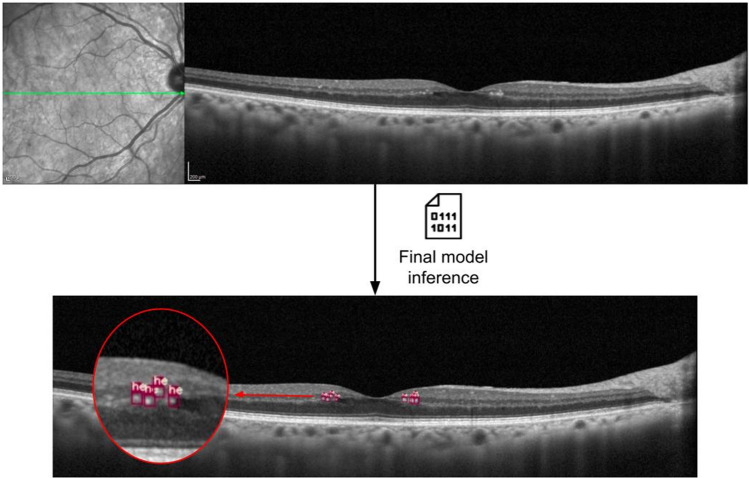
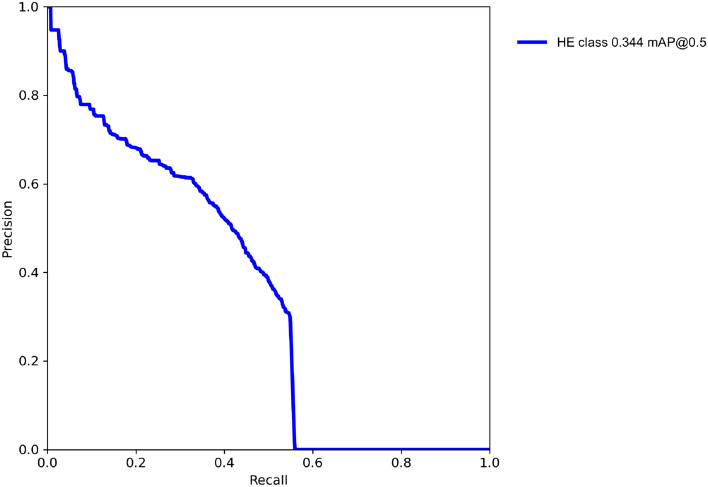
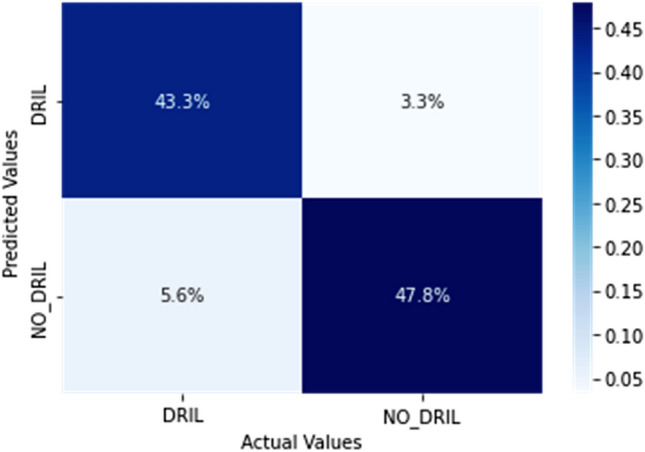
The purpose of the study was to detect Hard Exudates (HE) and classify Disorganization of Retinal Inner Layers (DRIL) implementing a Deep Learning (DL) system on optical coherence tomography (OCT) images of eyes with diabetic macular edema (DME). We collected a dataset composed of 442 OCT images on which we annotated 6847 HE and the presence of DRIL. A complex operational pipeline was defined to implement data cleaning and image transformations, and train two DL models. The state-of-the-art neural network architectures (Yolov7, ConvNeXt, RegNetX) and advanced techniques were exploited to aggregate the results (Ensemble learning, Edge detection) and obtain a final model. The DL approach reached good performance in detecting HE and classifying DRIL. Regarding HE detection the model got an AP@0.5 score equal to 34.4% with Precision of 48.7% and Recall of 43.1%; while for DRIL classification an Accuracy of 91.1% with Sensitivity and Specificity both of 91.1% and AUC and AUPR values equal to 91% were obtained. The P-value was lower than 0.05 and the Kappa coefficient was 0.82. The DL models proved to be able to identify HE and DRIL in eyes with DME with a very good accuracy and all the metrics calculated confirmed the system performance. Our DL approach demonstrated to be a good candidate as a supporting tool for ophthalmologists in OCT images analysis.
© 2024. The Author(s).
Conflict of interest statement
Lisa Toto, Anna Romano, Marco Pavan, Dante Degl’Innocenti, Valentina Olivotto, Federico Formenti, Pasquale Viggiano, Edoardo Midena and Rodolfo Mastropasqua declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
