

Clinicopathological discrepancies in the diagnoses of childhood causes of death in the CHAMPS network: An analysis of antemortem diagnostic inaccuracies
- PMID: 39032935
- PMCID: PMC11409330
- DOI: 10.1136/bmjpo-2024-002654
Clinicopathological discrepancies in the diagnoses of childhood causes of death in the CHAMPS network: An analysis of antemortem diagnostic inaccuracies
Abstract
Introduction: Determining aetiology of severe illness can be difficult, especially in settings with limited diagnostic resources, yet critical for providing life-saving care. Our objective was to describe the accuracy of antemortem clinical diagnoses in young children in high-mortality settings, compared with results of specific postmortem diagnoses obtained from Child Health and Mortality Prevention Surveillance (CHAMPS).
Methods: We analysed data collected during 2016-2022 from seven sites in Africa and South Asia. We compared antemortem clinical diagnoses from clinical records to a reference standard of postmortem diagnoses determined by expert panels at each site who reviewed the results of histopathological and microbiological testing of tissue, blood, and cerebrospinal fluid. We calculated test characteristics and 95% CIs of antemortem clinical diagnostic accuracy for the 10 most common causes of death. We classified diagnostic discrepancies as major and minor, per Goldman criteria later modified by Battle.
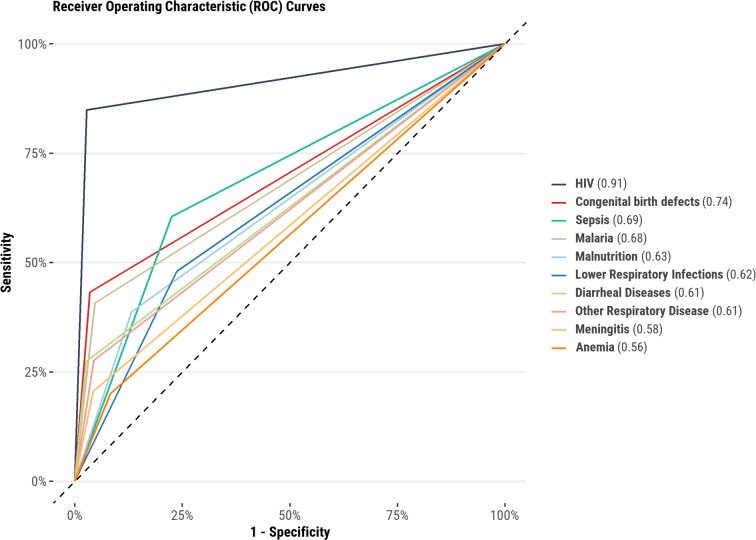
Results: CHAMPS enrolled 1454 deceased young children aged 1-59 months during the study period; 881 had available clinical records and were analysed. The median age at death was 11 months (IQR 4-21 months) and 47.3% (n=417) were female. We identified a clinicopathological discrepancy in 39.5% (n=348) of deaths; 82.3% of diagnostic errors were major. The sensitivity of clinician antemortem diagnosis ranged from 26% (95% CI 14.6% to 40.3%) for non-infectious respiratory diseases (eg, aspiration pneumonia, interstitial lung disease, etc) to 82.2% (95% CI 72.7% to 89.5%) for diarrhoeal diseases. Antemortem clinical diagnostic specificity ranged from 75.2% (95% CI 72.1% to 78.2%) for diarrhoeal diseases to 99.0% (95% CI 98.1% to 99.6%) for HIV.
Conclusions: Antemortem clinical diagnostic errors were common for young children who died in areas with high childhood mortality rates. To further reduce childhood mortality in resource-limited settings, there is an urgent need to improve antemortem diagnostic capability through advances in the availability of diagnostic testing and clinical skills.
Keywords: Child Health; Mortality.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- GBD 2019 Demographics Collaborators Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1160–203. doi: 10.1016/S0140-6736(20)30977-6. - DOI - PMC - PubMed
-
- World Health Organization Child mortality (under 5 years) 2022. [2-May-2023]. https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-ch... Available. Accessed.
-
- UNICEF Africa key facts and figures for child mortality. 2020. [21-Aug-2023]. https://data.unicef.org/resources/children-in-africa-child-survival-broc... Available. Accessed.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources