

Ultrasound-guided lesser occipital nerve combined with great auricular nerve block for vestibular schwannoma craniotomy via a suboccipital retrosigmoid approach: a prospective, double-blind randomized controlled trial
- PMID: 39033110
- PMCID: PMC11264943
- DOI: 10.1186/s12871-024-02642-2
Ultrasound-guided lesser occipital nerve combined with great auricular nerve block for vestibular schwannoma craniotomy via a suboccipital retrosigmoid approach: a prospective, double-blind randomized controlled trial
Abstract
Purpose: This aim of this study was to investigate the analgesic efficacy and safety of lesser occipital nerve combined with great auricular nerve block (LOGAB) for craniotomy via a suboccipital retrosigmoid approach.
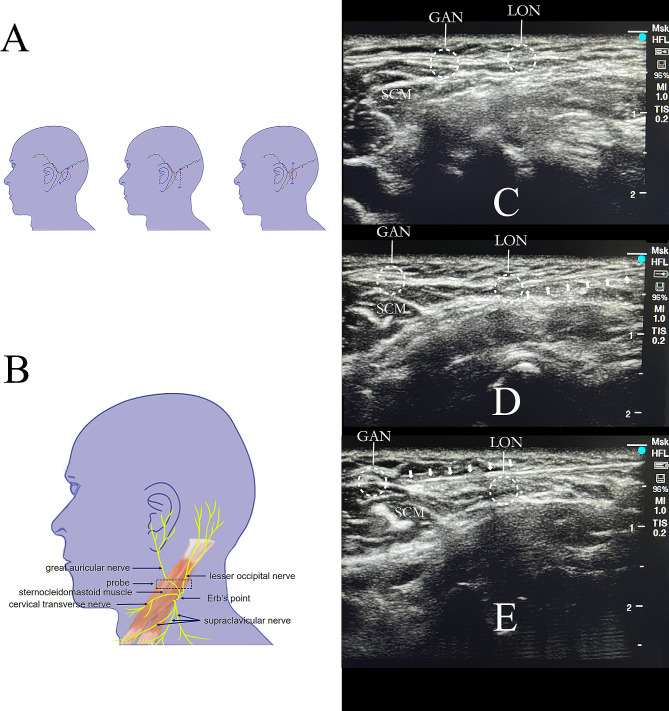
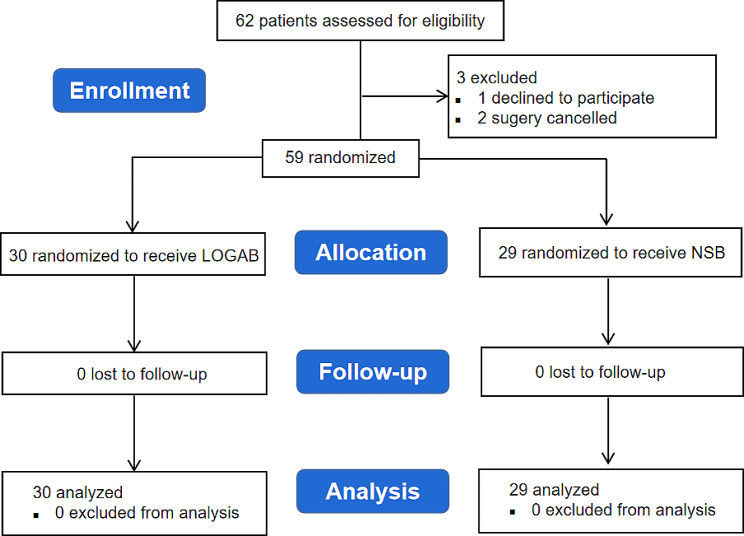
Methods: Patients underwent vestibular schwannoma resection via a suboccipital retrosigmoid approach were randomly assigned to receive ultrasound-guided unilateral LOGAB with 5 ml of 0.5% ropivacaine (LOGAB group) or normal saline (NSB group). Numeric rating scale (NRS) scores at rest and motion were recorded within 48 h after surgery. Mean arterial pressure (MAP), heart rate (HR), opioid consumption and other variables were measured secondly.
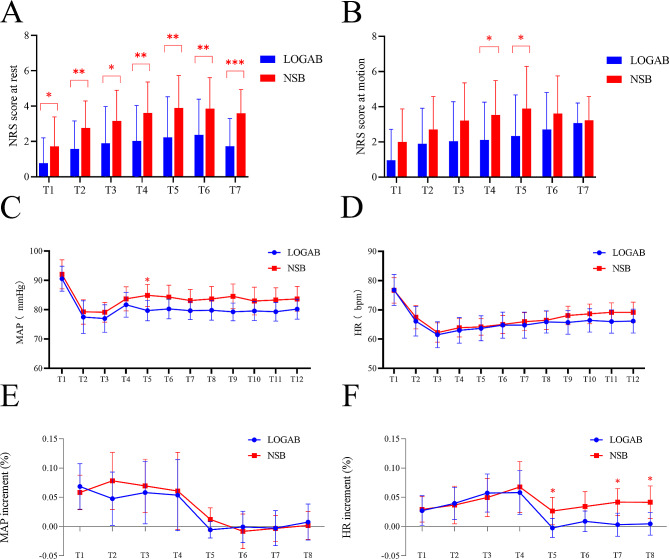
Results: Among 59 patients who were randomized, 30 patients received ropivacaine, and 29 patients received saline. NRS scores at rest (1.8 ± 0.5 vs. 3.2 ± 0.8, P = 0.002) and at motion (2.2 ± 0.7 vs. 3.2 ± 0.6, P = 0.013) of LOGAB group were lower than those of NSB group within 48 h after surgery. NRS scores of motion were comparable except for 6th and 12th hour (P < 0.05) in the LOGAB group. In LOGAB group, MAP decreased significantly during incision of skin and dura (P < 0.05) and intraoperative opoid consumption was remarkably reduced (P < 0.01). Postoperative remedial analgesia was earlier in the NSB group (P < 0.001). No patients reported any adverse events.
Conclusion: Among patients undergoing craniotomy for vestibular schwannoma via a suboccipital retrosigmoid approach, LOGAB may be a promising treatment for perioperative analgesia and has the potential to maintain intraoperative hemodynamic stability.
Clinical trial registration number: Chictr.org.cn ChiCTR2000038798.
Keywords: Great auricular nerve block; Lesser occipital nerve block; Suboccipital retrosigmoid craniotomy; Ultrasound-guided; Vestibular schwannoma resection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The analgesic efficacy of subcostal transversus abdominis plane block with Mercedes incision.BMC Anesthesiol. 2018 Apr 10;18(1):36. doi: 10.1186/s12871-018-0499-3. BMC Anesthesiol. 2018. PMID: 29631564 Free PMC article. Clinical Trial.
-
Postoperative analgesia of scalp nerve block with ropivacaine in pediatric craniotomy patients: a protocol for a prospective, randomized, placebo-controlled, double-blinded trial.Trials. 2020 Jun 26;21(1):580. doi: 10.1186/s13063-020-04524-7. Trials. 2020. PMID: 32586348 Free PMC article.
-
Analgesic efficacy of postoperative bilateral, ultrasound-guided, posterior transversus abdominis plane block for laparoscopic colorectal cancer surgery: a randomized, prospective, controlled study.BMC Anesthesiol. 2021 Apr 6;21(1):107. doi: 10.1186/s12871-021-01317-6. BMC Anesthesiol. 2021. PMID: 33823786 Free PMC article. Clinical Trial.
-
Ultrasound-guided erector spinae plane block for postoperative analgesia in patients undergoing minimally invasive direct coronary artery bypass surgery: a double-blinded randomized controlled trial.Can J Anaesth. 2024 Jun;71(6):784-792. doi: 10.1007/s12630-023-02637-6. Epub 2023 Nov 21. Can J Anaesth. 2024. PMID: 37989939 Free PMC article. Clinical Trial.
-
An overview of definition and approaches to jugular fossa tumors.Langenbecks Arch Surg. 2025 Jul 1;410(1):207. doi: 10.1007/s00423-025-03794-6. Langenbecks Arch Surg. 2025. PMID: 40591002 Free PMC article. Review.
References
-
- De Benedittis G, Lorenzetti A, Migliore M, Spagnoli D, Tiberio F, Villani RM. Postoperative pain in neurosurgery: a pilot study in brain surgery. Neurosurgery. 1996;38(3):466–9. discussion 469–470. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
