

SOD1 inhibition enhances sorafenib efficacy in HBV-related hepatocellular carcinoma by modulating PI3K/Akt/mTOR pathway and ROS-mediated cell death
- PMID: 39034442
- PMCID: PMC11260765
- DOI: 10.1111/jcmm.18533
SOD1 inhibition enhances sorafenib efficacy in HBV-related hepatocellular carcinoma by modulating PI3K/Akt/mTOR pathway and ROS-mediated cell death
Abstract
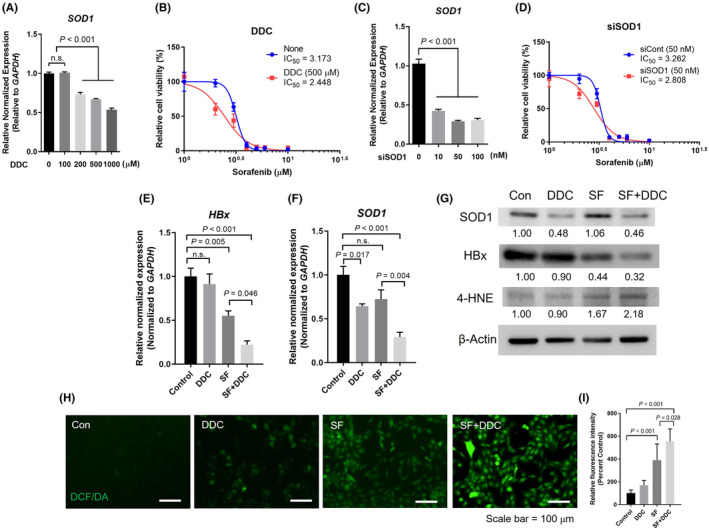
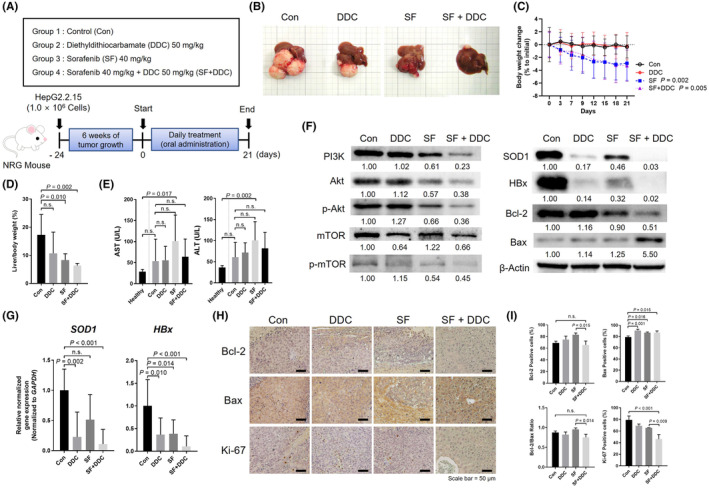
Hepatitis B Virus (HBV) infection significantly elevates the risk of hepatocellular carcinoma (HCC), with the HBV X protein (HBx) playing a crucial role in cancer progression. Sorafenib, the primary therapy for advanced HCC, shows limited effectiveness in HBV-infected patients due to HBx-related resistance. Numerous studies have explored combination therapies to overcome this resistance. Sodium diethyldithiocarbamate (DDC), known for its anticancer effects and its inhibition of superoxide dismutase 1 (SOD1), is hypothesized to counteract sorafenib (SF) resistance in HBV-positive HCCs. Our research demonstrates that combining DDC with SF significantly reduces HBx and SOD1 expressions in HBV-positive HCC cells and human tissues. This combination therapy disrupts the PI3K/Akt/mTOR signalling pathway and promotes apoptosis by increasing reactive oxygen species (ROS) levels. These cellular changes lead to reduced tumour viability and enhanced sensitivity to SF, as evidenced by the synergistic suppression of tumour growth in xenograft models. Additionally, DDC-mediated suppression of SOD1 further enhances SF sensitivity in HBV-positive HCC cells and xenografted animals, thereby inhibiting cancer progression more effectively. These findings suggest that the DDC-SF combination could serve as a promising strategy for overcoming SF resistance in HBV-related HCC, potentially optimizing therapy outcomes.
Keywords: Sorafenib resistance; disulfiram; hepatitis B virus; hepatocellular carcinoma; superoxide dismutase.
© 2024 The Author(s). Journal of Cellular and Molecular Medicine published by Foundation for Cellular and Molecular Medicine and John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
