

Difficulty in Early Diagnosis of Bilateral Posterior Fracture-dislocation of the Shoulder Caused by an Electric Shock in a Walk-in Patient: A Case Report
- PMID: 39035384
- PMCID: PMC11258722
- DOI: 10.13107/jocr.2024.v14.i07.4564
Difficulty in Early Diagnosis of Bilateral Posterior Fracture-dislocation of the Shoulder Caused by an Electric Shock in a Walk-in Patient: A Case Report
Abstract
Introduction: Bilateral posterior fracture-dislocation of the shoulder is a very rare injury that is commonly missed. Almost 70% of bilateral posterior dislocations are due to convulsive seizures, with electric shocks accounting for < 5% of bilateral posterior shoulder dislocations.
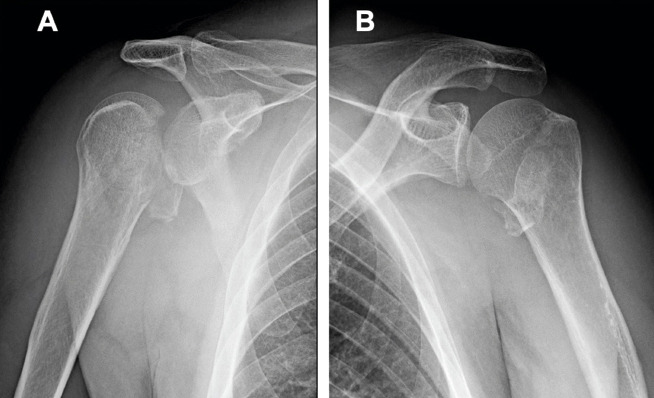
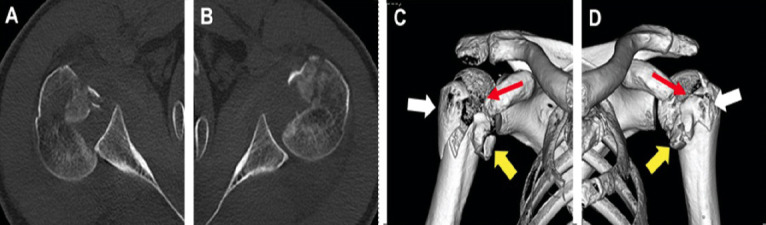
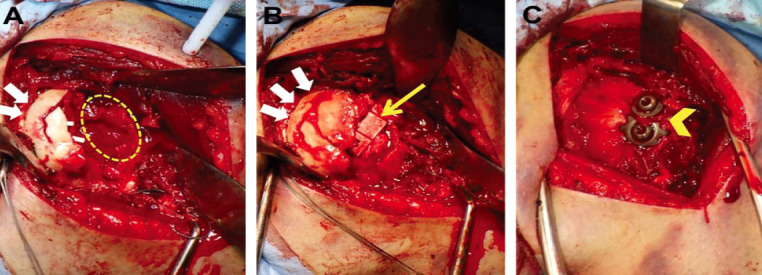
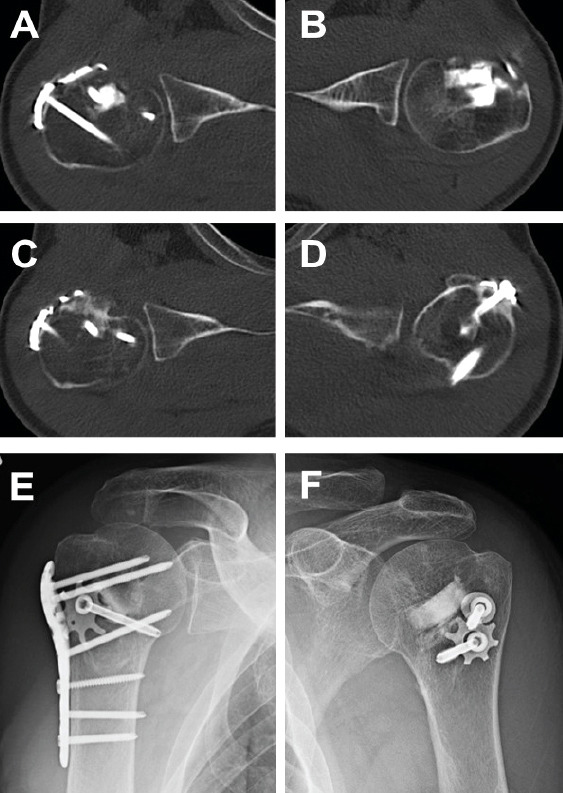
Case report: The case of a walk-in patient, a 52-year-old man, with bilateral posterior fracture-dislocation of the shoulder caused by an electric shock is reported. Although he was initially admitted to the emergency department for observation of the potential complications of an electric shock, such as fatal arrhythmia and rhabdomyolysis, he subsequently consulted an orthopedic surgeon 4 days after the event due to persistent bilateral shoulder pain and was diagnosed using X-ray and computed tomography with bilateral posterior fracture-dislocation of the shoulder. Following open reduction and internal fixation 7 days after the injury, the upper limbs were fixed with shoulder braces at a slightly flexed and abducted position with neutral rotation for 3 weeks postoperatively followed by range of motion exercises. Twelve months after surgery, he had a Constant shoulder score of 94, an American Shoulder and Elbow Surgeon score of 100, and no shoulder re-dislocation or humeral head necrosis.
Conclusion: In this walk-in patient, the diagnosis of bilateral posterior fracture-dislocation of the shoulder caused by an electric shock was delayed. We believe that understanding the mechanism of this type of injury will facilitate its early diagnosis.
Keywords: Bilateral; electric shock; posterior fracture-dislocation; shoulder.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures
Similar articles
-
Bilateral posterior fracture-dislocation of the shoulders: Two rare case reports and literature review.Medicine (Baltimore). 2020 Sep 4;99(36):e22088. doi: 10.1097/MD.0000000000022088. Medicine (Baltimore). 2020. PMID: 32899086 Free PMC article.
-
Bilateral posterior shoulder dislocation after electrical shock: A case report.Ann Med Surg (Lond). 2015 Nov 4;4(4):417-21. doi: 10.1016/j.amsu.2015.10.010. eCollection 2015 Dec. Ann Med Surg (Lond). 2015. PMID: 26904192 Free PMC article.
-
Asymmetrical Fracture Dislocation of Shoulder - A Case Report and Review of Literature.J Orthop Case Rep. 2013 Oct-Dec;3(4):19-22. doi: 10.13107/jocr.2250-0685.125. J Orthop Case Rep. 2013. PMID: 27298925 Free PMC article.
-
Bilateral Locked Posterior Fracture-Dislocation of the Shoulder After Epileptic Seizures Secondary to Cavernous Hemangioma: A Case Report and Literature Review.Am J Case Rep. 2023 Jun 19;24:e940141. doi: 10.12659/AJCR.940141. Am J Case Rep. 2023. PMID: 37337276 Free PMC article. Review.
-
Posterior shoulder fracture-dislocation: an update with treatment algorithm.Eur J Orthop Surg Traumatol. 2017 Apr;27(3):285-294. doi: 10.1007/s00590-016-1840-5. Epub 2016 Aug 25. Eur J Orthop Surg Traumatol. 2017. PMID: 27562590 Review.
References
-
- Brackstone M, Patterson SD, Kertesz A. Triple “E”syndrome:Bilateral locked posterior fracture dislocation of the shoulders. Neurology. 2001;56:1403–4. - PubMed
-
- Huizing JW, Monteban PE. Bilateral posterior fracture dislocation of the shoulders:Review of case reports and treatment. Acta Orthop Belg. 2020;86:193–9. - PubMed
-
- Rowe CR, Zarins B. Chronic unreduced dislocations of the shoulder. J Bone Joint Surg Am. 1982;64:494–505. - PubMed
-
- Hawkins RJ, Neer CS, 2nd, Pianta RM, Mendoza FX. Locked posterior dislocation of the shoulder. J Bone Joint Surg Am. 1987;69:9–18. - PubMed
Publication types
LinkOut - more resources
Full Text Sources