

Efficacy and Safety of Pharmacokinetically-Driven Dosing of Mycophenolate Mofetil for the Treatment of Pediatric Proliferative Lupus Nephritis-A Double-Blind Placebo Controlled Clinical Trial (The Pediatric Lupus Nephritis Mycophenolate Mofetil Study)
- PMID: 39035447
- PMCID: PMC11258879
Efficacy and Safety of Pharmacokinetically-Driven Dosing of Mycophenolate Mofetil for the Treatment of Pediatric Proliferative Lupus Nephritis-A Double-Blind Placebo Controlled Clinical Trial (The Pediatric Lupus Nephritis Mycophenolate Mofetil Study)
Abstract
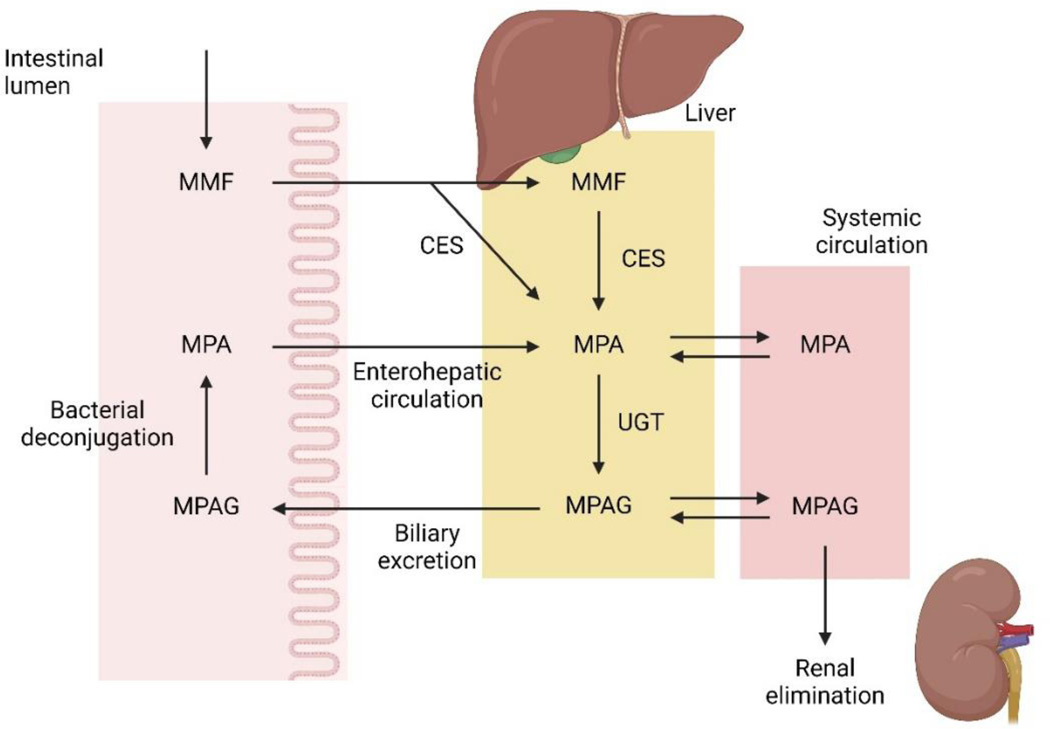
Background: The safety and efficacy of mycophenolate mofetil (MMF) for lupus nephritis (LN) treatment is established in adults and in some children. MMF is rapidly converted to the biologically active metabolite mycophenolic acid (MPA) whose pharmacokinetics (PK) is characterized by large inter- and intra-individual variability.
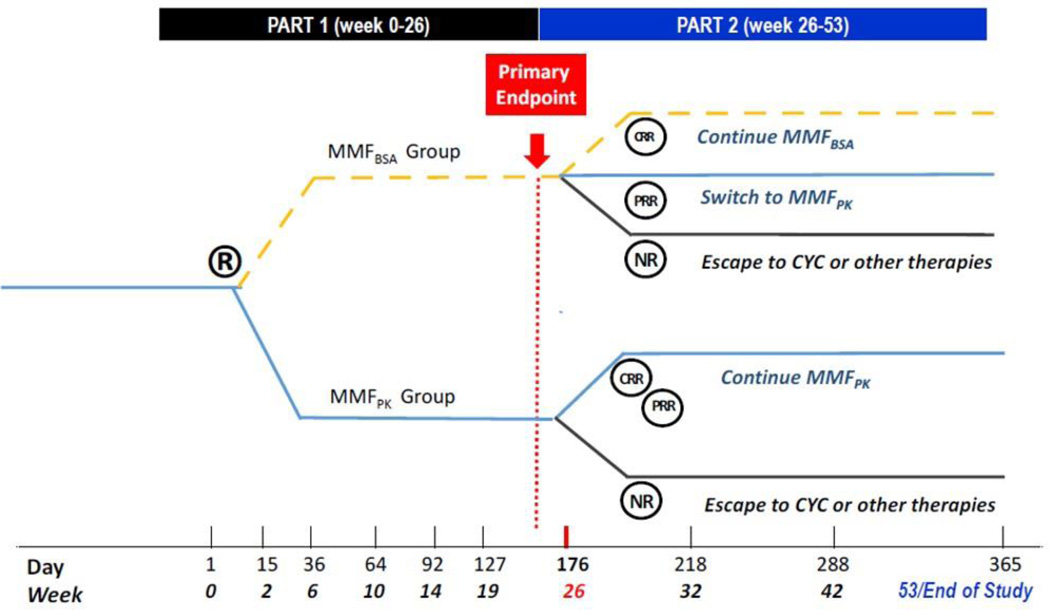
Methods/design: This randomized, double-blind, active comparator, controlled clinical trial of pediatric subjects with proliferative LN compares pharmacokinetically-guided precision-dosing of MMF (MMFPK, i.e. the dose is adjusted to the target area under the concentration-time curve (AUC0-12h) of MPA ≥ 60-70 mg*h/L) and MMF dosed per body surface area (MMFBSA, i.e. MMF dosed 600 mg/m2 body surface area), with MMF dosage taken about 12 hours apart. At baseline, subjects are randomized 1:1 to receive blinded treatment with MMFPK or MMFBSA for up to 53 weeks. The primary outcome is partial clinical remission of LN (partial renal response, PRR) at week 26, and the major secondary outcome is complete renal response (CRR) at week 26. Subjects in the MMFBSA arm with PRR at week 26 will receive MMFPK from week 26 onwards, while subjects with CRR will continue MMFBSA or MMFPK treatment until week 53. Subjects who achieve PRR at week 26 are discontinued from study intervention.
Discussion: The Pediatric Lupus Nephritis Mycophenolate Mofetil (PLUMM) study will provide a thorough evaluation of the PK of MMF in pediatric LN patients, yielding a head-to-head comparison of MMFBSA and MMFPK for both safety and efficacy. This study has the potential to change current treatment recommendations for pediatric LN, thereby significantly impacting childhood-onset SLE (cSLE) disease prognosis and current clinical practice.
Keywords: Childhood-onset; Lupus; Lupus nephritis; Mycophenolate mofetil; Pediatric; Pharmacokinetics; SLE.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources