

Immunotherapy in breast cancer: A clinician's perspective
- PMID: 39035768
- PMCID: PMC11256727
- DOI: 10.1016/j.jncc.2021.01.001
Immunotherapy in breast cancer: A clinician's perspective
Abstract
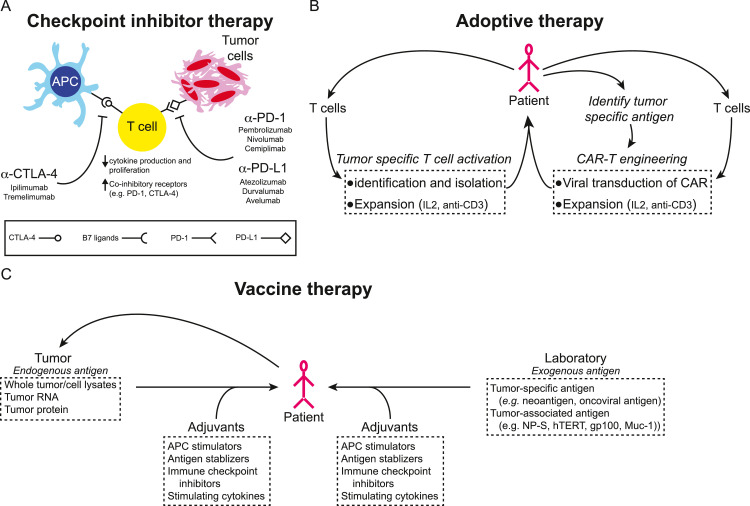
Globally over 2 million women are diagnosed with breast cancer each year despite major advances in detection and treatment of the disease. Breast cancer is comprised of several distinct subtypes and understanding the heterogeneity of the disease has become crucial for treatment planning. Therapeutic strategies span from a hormone therapy-based focus for women with estrogen receptor positive breast cancer to targeting human epidermal growth factor (HER2) by small molecules, antibody-drug-conjugates (ADC) and monoclonal antibodies in those with HER2 overexpression. Other novel treatment strategies for select subgroups of patients include the cyclin-dependent kinase 4/6 (CDK4/6) inhibitors for women with estrogen receptor positive tumors, the poly ADP ribose polymerase (PARP) inhibitors for those with BRCA mutations, and phosphoinositide 3-kinase (PI3K) inhibitors for women with tumors harboring phophatidylinositol-4,5-bisphosphate 3 kinase catalytic subunit alpha (PIK3CA) mutations. In contrast, the treatment for women with triple negative breast cancer has until recently been solely limited to chemotherapy. The profound impact of immunotherapy on cancer treatment in general has created much hope for its potential in breast cancer. This review will focus on the current advances and the research of immunotherapy in breast cancer, particularly on immune checkpoint inhibitors, adoptive cell transfer and cancer vaccines.
© 2019 Chinese National Cancer Center. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures

Similar articles
-
Novel combinatorial strategies for boosting the efficacy of immune checkpoint inhibitors in advanced breast cancers.Clin Transl Oncol. 2021 Oct;23(10):1979-1994. doi: 10.1007/s12094-021-02613-w. Epub 2021 Apr 19. Clin Transl Oncol. 2021. PMID: 33871826 Review.
-
Breast cancer: an up-to-date review and future perspectives.Cancer Commun (Lond). 2022 Oct;42(10):913-936. doi: 10.1002/cac2.12358. Epub 2022 Sep 8. Cancer Commun (Lond). 2022. PMID: 36074908 Free PMC article. Review.
-
Advances in Therapy for Hormone Receptor (HR)-Positive, Human Epidermal Growth Factor Receptor 2 (HER2)-Negative Advanced Breast Cancer Patients Who Have Experienced Progression After Treatment with CDK4/6 Inhibitors.Onco Targets Ther. 2021 May 3;14:2929-2939. doi: 10.2147/OTT.S298720. eCollection 2021. Onco Targets Ther. 2021. PMID: 33976551 Free PMC article. Review.
-
Optimizing the management of HER2-negative metastatic breast cancer in the era of PARP inhibitors-proceedings from breast cancer expert group meeting.Chin Clin Oncol. 2020 Oct;9(5):61. doi: 10.21037/cco-20-138. Epub 2020 Aug 17. Chin Clin Oncol. 2020. PMID: 32819114 Review.
-
Advances in Targeted Therapies for Triple-Negative Breast Cancer.Drugs. 2019 Jul;79(11):1217-1230. doi: 10.1007/s40265-019-01155-4. Drugs. 2019. PMID: 31254268 Review.
Cited by
-
ETV7 reduces inflammatory responses in breast cancer cells by repressing the TNFR1/NF-κB axis.Cell Death Dis. 2023 Apr 12;14(4):263. doi: 10.1038/s41419-023-05718-y. Cell Death Dis. 2023. PMID: 37041130 Free PMC article.
-
Modulation of the tumor microenvironment and mechanism of immunotherapy-based drug resistance in breast cancer.Mol Cancer. 2024 May 7;23(1):92. doi: 10.1186/s12943-024-01990-4. Mol Cancer. 2024. PMID: 38715072 Free PMC article. Review.
-
Peripheral Blood Transcriptome in Breast Cancer Patients as a Source of Less Invasive Immune Biomarkers for Personalized Medicine, and Implications for Triple Negative Breast Cancer.Cancers (Basel). 2022 Jan 25;14(3):591. doi: 10.3390/cancers14030591. Cancers (Basel). 2022. PMID: 35158858 Free PMC article. Review.
-
Current Immunotherapy Treatments of Primary Breast Cancer Subtypes.Biomedicines. 2024 Apr 18;12(4):895. doi: 10.3390/biomedicines12040895. Biomedicines. 2024. PMID: 38672249 Free PMC article. Review.
-
Reconstruction of the tumor spatial microenvironment along the malignant-boundary-nonmalignant axis.Nat Commun. 2023 Feb 20;14(1):933. doi: 10.1038/s41467-023-36560-7. Nat Commun. 2023. PMID: 36806082 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
