

All-cause and AIDS-related mortality among people with HIV across Europe from 2001 to 2020: impact of antiretroviral therapy, tuberculosis and regional differences in a multicentre cohort study
- PMID: 39036304
- PMCID: PMC11259909
- DOI: 10.1016/j.lanepe.2024.100989
All-cause and AIDS-related mortality among people with HIV across Europe from 2001 to 2020: impact of antiretroviral therapy, tuberculosis and regional differences in a multicentre cohort study
Abstract
Background: All-cause and AIDS-mortality in Europe has been decreasing between 1996 and 2020. However, regional differences as well as their drivers remain unclear. This study investigates mortality differences and their drivers, including usage of and response to antiretroviral therapy (ART) and active tuberculosis (TB), among people with HIV across Europe.
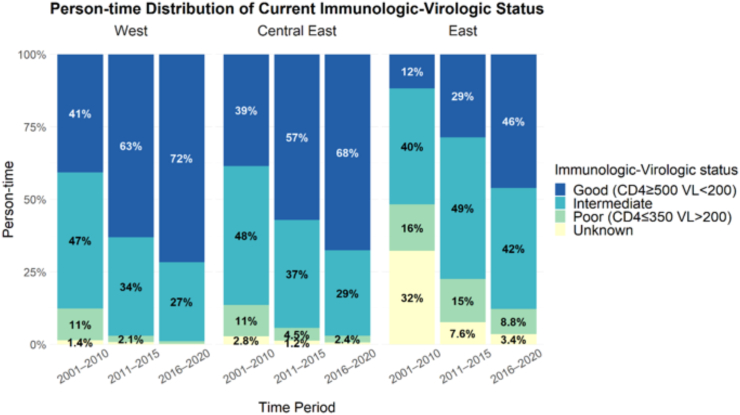
Methods: People with HIV enrolled in EuroSIDA were followed from 2001 through 2020. Immunologic-virologic status (IVS) was categorized as poor (CD4-cell count ≤350 cells/mm3 and viral load (VL) > 200 copies/ml), good (CD4 ≥ 500 and VL < 200), or intermediate (remaining combinations). Participants missing either CD4-cell count or VL were categorized as unknown. Regional differences in mortality were analyzed using multivariable Poisson regression with interaction analyses between regions of Europe and IVS, ART, or TB status.
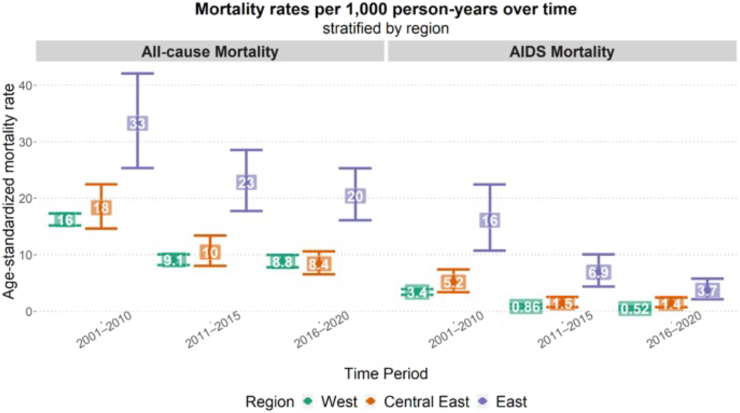
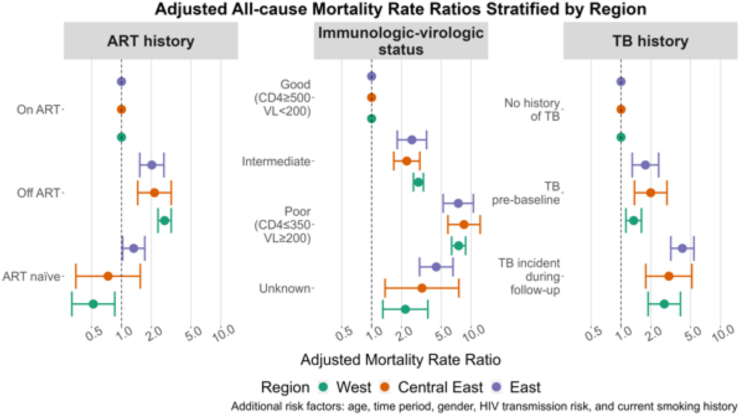
Findings: 20,364 people with HIV were included: 13,715/20,346 (67.3%) from Western, 3020/20,364 (14.8%) from Central Eastern, and 3629/20,364 (17.8%) from Eastern Europe. At enrolment, median age was 40 years (inter-quartile range (IQR): 33-48), median CD4-cell count 449 cells/mm3 (IQR: 291-638), and most were male 14,993/20,346 (73.3%). A total of 2639 died during 192,591 person-years of follow-up (crude mortality rate 13.7/1000 person-years, 95% CI: 13.2-14.2), 519/2639 (19.7%) from AIDS (2.7/1000 person-years, 2.5-2.9). All-cause and AIDS-mortality rates decreased over time but remained higher in Eastern Europe after adjusting for confounders. Being off ART (aIRR 2.42; 95% CI 2.14-2.74), poor IVS (aIRR 4.2; 95% CI 3.39-5.20) and prior TB (aIRR 3.33; 95% CI 2.75-4.03) were associated with higher all-cause mortality. For all-cause mortality the effect of ART (test for interaction: p < 0.001) and IVS (p = 0.02), but not TB (p = 0.5) varied across regions.
Interpretation: Overall mortality and AIDS-mortality rates decreased over time, but remained higher in Eastern Europe. A poor IVS, being off ART and prior active TB were related to higher mortality. Eastern Europe had the highest proportion of people with poor or unknown IVS, emphasizing the continued need to improve HIV care with a focus on early diagnosis, ART initiation, and adherence.
Funding: EuroSIDA has received funding from ViiV Healthcare LLC, Janssen Scientific Affairs, Janssen R&D, Bristol-Myers Squibb Company, Merck Sharp & Dohme Corp, Gilead Sciences and the European Union's Seventh Framework Programme for research, technological development and demonstration under EuroCoord grant agreement n˚ 260694. The study is also supported by a grant from the Danish National Research Foundation and by the International Cohort Consortium of Infectious Disease (RESPOND).
Keywords: AIDS; ART; Eastern Europe; Europe; HIV; Healthcare; Mortality; Tuberculosis.
© 2024 The Author(s).
Conflict of interest statement
OK, BS, AC, GM have research grants, personal fees for lectures and consultancy, meeting support from Gilead, MSD and ViiV outside the submitted work. AC has received consulting fees participation on data monitoring board, personal fees for lectures and consultancy, meeting support from Gilead, MSD Jannsen Cilag and ViiV outside the submitted work. CK received payment for a lecture from Gilead outside the submitted work. ET, SS, LØ, GF, SM, KK, AK, JT, JR, RZ, FM, SW, JG, DP, LP, and JR declare no competing interests.
Figures
References
-
- Fursa O. 2023. Temporal trends and impact of COVID-19 on the HIV cascade of care across Europe between 2016-2021. Warsaw, Poland.
-
- Chiesi A., Mocroft A., Dally L.G., et al. Regional survival differences across Europe in HIV-positive people: the EuroSIDA study. AIDS. 1999;13:2281–2288. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
