

Association between Chronic Kidney Disease-Mineral and Bone Disorder Biomarkers and Symptom Burden in Older Patients with Advanced Chronic Kidney Disease: Results from the EQUAL Study
- PMID: 39037951
- PMCID: PMC11469787
- DOI: 10.2215/CJN.0000000000000510
Association between Chronic Kidney Disease-Mineral and Bone Disorder Biomarkers and Symptom Burden in Older Patients with Advanced Chronic Kidney Disease: Results from the EQUAL Study
Abstract
Key Points:
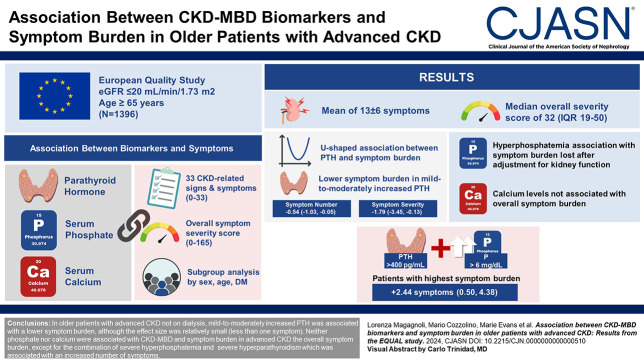
In nondialysis patients with advanced CKD, mild-to-moderately increased parathyroid hormone is associated with lower levels of reported symptoms.
Phosphate and calcium are not independently associated with overall symptom burden.
Patients with both severe hyperphosphatemia and severe hyperparathyroidism had the highest symptom burden.
Background: Patients with advanced CKD develop numerous symptoms, with a multifactorial origin. Evidence linking mineral disorders (CKD-Mineral and Bone Disorder) and uremic symptoms is scant and mostly limited to dialysis patients. Here, we aim to assess the association between CKD-Mineral and Bone Disorder and symptom burden in nondialysis patients with CKD.
Methods: We used data from the European Quality study, which includes patients aged ≥65 years with eGFR ≤20 ml/min per 1.73 m2 from six European countries, followed up to 5 years. We used generalized linear mixed-effect models to determine the association between repeated measurements of parathyroid hormone (PTH), phosphate, and calcium with the overall symptom number (0–33), the overall symptom severity (0–165), and the presence of 33 CKD-related symptoms. We also analyzed subgroups by sex, age, and diabetes mellitus and assessed effect mediation and joint effects between mineral biomarkers.
Results: The 1396 patients included in the study had a mean of 13±6 symptoms at baseline, with a median overall severity score of 32 (interquartile range, 19–50). The association between PTH levels and symptom burden appeared U-shaped with a lower symptom burden found for mild-to-moderately increased PTH levels. Phosphate and calcium were not independently associated with overall symptom burden. The highest symptom burden was found in patients with a combination of both severe hyperparathyroidism and severe hyperphosphatemia (+2.44 symptoms [0.50–4.38], P = 0.01). The association of both hypocalcemia and hyperphosphatemia with symptom burden seemed to differ by sex and age.
Conclusions: In older patients with advanced CKD not on dialysis, mild-to-moderately increased PTH was associated with a lower symptom burden, although the effect size was relatively small (less than one symptom). Neither phosphate nor calcium were associated with the overall symptom burden, except for the combination of severe hyperphosphatemia and severe hyperparathyroidism which was associated with an increased number of symptoms.
Conflict of interest statement
Disclosure forms, as provided by each author, are available with the online version of the article at
Figures





References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
