

Conventional magnetic resonance imaging key features for distinguishing pathologically confirmed corticobasal degeneration from its mimics: a retrospective analysis of the J-VAC study
- PMID: 39039147
- PMCID: PMC11535003
- DOI: 10.1007/s00234-024-03432-w
Conventional magnetic resonance imaging key features for distinguishing pathologically confirmed corticobasal degeneration from its mimics: a retrospective analysis of the J-VAC study
Abstract
Purpose: Due to the indistinguishable clinical features of corticobasal syndrome (CBS), the antemortem differentiation between corticobasal degeneration (CBD) and its mimics remains challenging. However, the utility of conventional magnetic resonance imaging (MRI) for the diagnosis of CBD has not been sufficiently evaluated. This study aimed to investigate the diagnostic performance of conventional MRI findings in differentiating pathologically confirmed CBD from its mimics.
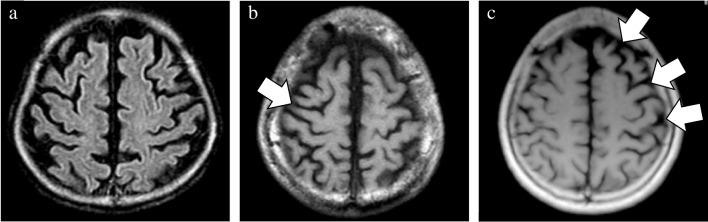
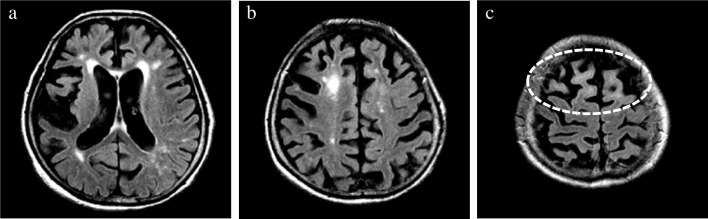
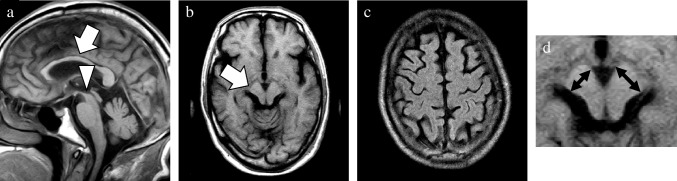
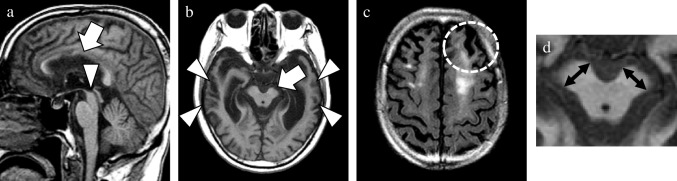
Methods: Semiquantitative visual rating scales were employed to assess the degree and distribution of atrophy and asymmetry on conventional T1-weighted and T2-weighted images. Additionally, subcortical white matter hyperintensity (SWMH) on fluid-attenuated inversion recovery images were visually evaluated.
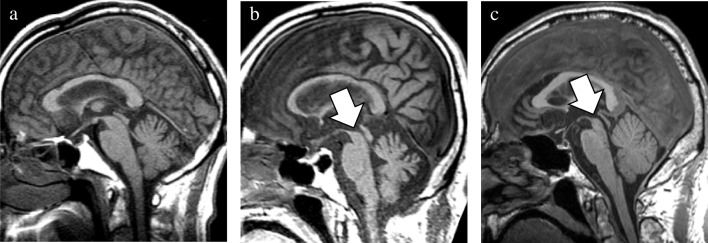
Results: In addition to 19 patients with CBD, 16 with CBD mimics (progressive supranuclear palsy (PSP): 9, Alzheimer's disease (AD): 4, dementia with Lewy bodies (DLB): 1, frontotemporal lobar degeneration with TAR DNA-binding protein of 43 kDa(FTLD-TDP): 1, and globular glial tauopathy (GGT): 1) were investigated. Compared with the CBD group, the PSP-CBS subgroup showed severe midbrain atrophy without SWMH. The non-PSP-CBS subgroup, comprising patients with AD, DLB, FTLD-TDP, and GGT, showed severe temporal atrophy with widespread asymmetry, especially in the temporal lobes. In addition to over half of the patients with CBD, two with FTLD-TDP and GGT showed SWMH, respectively.
Conclusion: This study elucidates the distinct structural changes between the CBD and its mimics based on visual rating scales. The evaluation of atrophic distribution and SWMH may serve as imaging biomarkers of conventional MRI for detecting background pathologies.
Keywords: Asymmetry; Corticobasal degeneration; Corticobasal syndrome; Magnetic resonance imaging; Subcortical white matter hyperintensity.
© 2024. The Author(s).
Conflict of interest statement
The authors declared that they have no competing interests.
Figures




References
-
- Dickson DW, Bergeron C, Chin SS, Duyckaerts C, Horoupian D, Ikeda K, Jellinger K, Lantos PL, Lippa CF, Mirra SS, Tabaton M, Vonsattel JP, Wakabayashi K, Litvan I (2002) Office of Rare Diseases neuropathologic criteria for corticobasal degeneration. J Neuropathol Exp Neurol 61(11):935–946. 10.1093/jnen/61.11.935 - PubMed
-
- Hattori M, Hashizume Y, Yoshida M, Iwasaki Y, Hishikawa N, Ueda R, Ojika K (2003) Distribution of astrocytic plaques in the corticobasal degeneration brain and comparison with tuft-shaped astrocytes in the progressive supranuclear palsy brain. Acta Neuropathol 106(2):143–149. 10.1007/s00401-003-0711-4 - PubMed
-
- Rohrer JD (2012) Structural brain imaging in frontotemporal dementia. Biochem Biophys Acta 1822(3):325–332. 10.1016/j.bbadis.2011.07.014 - PubMed
-
- Armstrong MJ, Litvan I, Lang AE, Bak TH, Bhatia KP, Borroni B, Boxer AL, Dickson DW, Grossman M, Hallett M, Josephs KA, Kertesz A, Lee SE, Miller BL, Reich SG, Riley DE, Tolosa E, Tröster AI, Vidailhet M, Weiner WJ (2013) Criteria for the diagnosis of corticobasal degeneration. Neurology 80(5):496–503. 10.1212/WNL.0b013e31827f0fd1 - PMC - PubMed
-
- Ling H, O’Sullivan SS, Holton JL, Revesz T, Massey LA, Williams DR, Paviour DC, Lees AJ (2010) Does corticobasal degeneration exist? A clinicopathological re-evaluation. Brain : a journal of neurology 133(Pt 7):2045–2057. 10.1093/brain/awq123 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
