

An outcome-driven threshold for pulse pressure amplification
- PMID: 39039284
- PMCID: PMC11374666
- DOI: 10.1038/s41440-024-01779-4
An outcome-driven threshold for pulse pressure amplification
Abstract
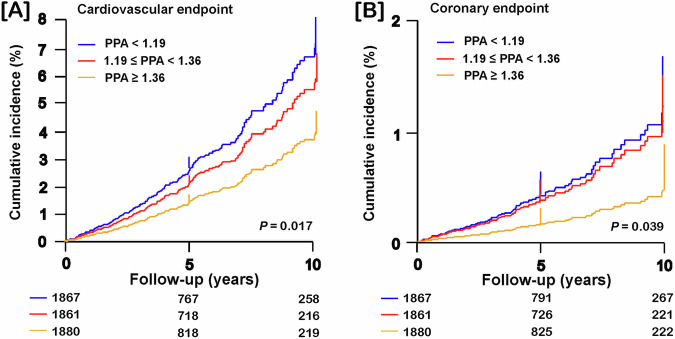
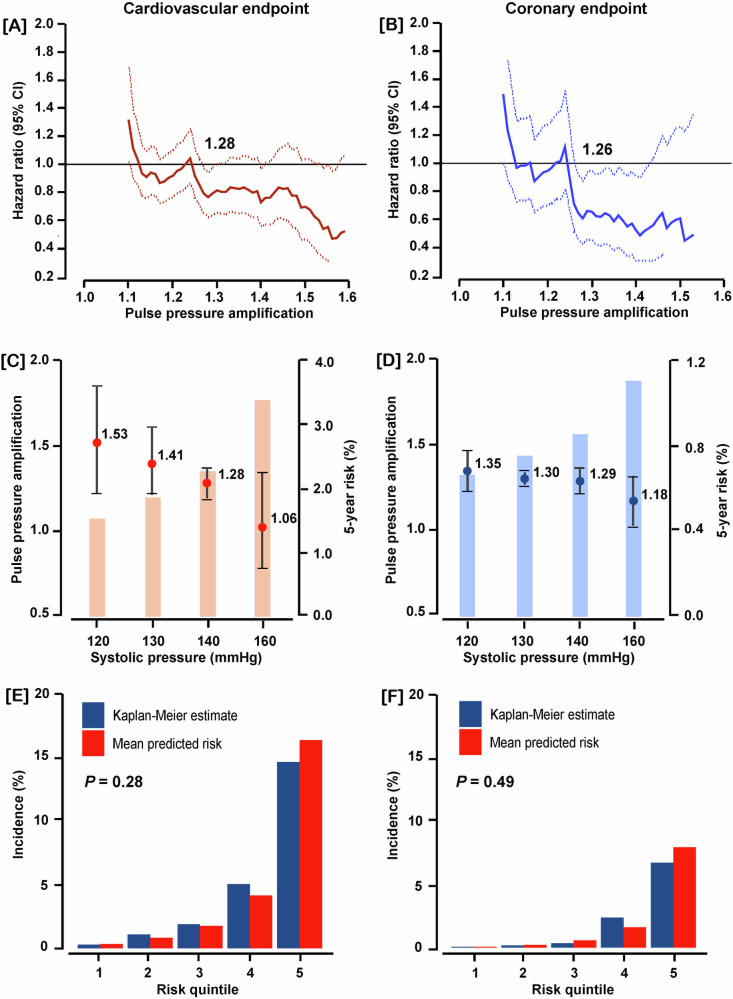
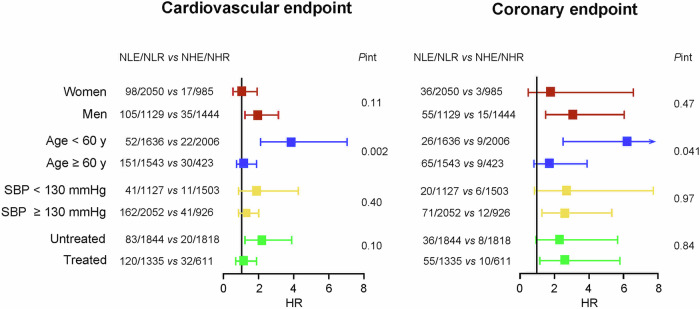
Pulse pressure amplification (PPA) is the brachial-to-aortic pulse pressure ratio and decreases with age and cardiovascular risk factors. This individual-participant meta-analysis of population studies aimed to define an outcome-driven threshold for PPA. Incidence rates and standardized multivariable-adjusted hazard ratios (HRs) of cardiovascular and coronary endpoints associated with PPA, as assessed by the SphygmoCor software, were evaluated in the International Database of Central Arterial Properties for Risk Stratification (n = 5608). Model refinement was assessed by the integrated discrimination (IDI) and net reclassification (NRI) improvement. Age ranged from 30 to 96 years (median 53.6). Over 4.1 years (median), 255 and 109 participants experienced a cardiovascular or coronary endpoint. In a randomly defined discovery subset of 3945 individuals, the rounded risk-carrying PPA thresholds converged at 1.3. The HRs for cardiovascular and coronary endpoints contrasting PPA < 1.3 vs ≥1.3 were 1.54 (95% confidence interval [CI]: 1.00-2.36) and 2.45 (CI: 1.20-5.01), respectively. Models were well calibrated, findings were replicated in the remaining 1663 individuals analyzed as test dataset, and NRI was significant for both endpoints. The HRs associating cardiovascular and coronary endpoints per PPA threshold in individuals <60 vs ≥60 years were 3.86 vs 1.19 and 6.21 vs 1.77, respectively. The proportion of high-risk women (PPA < 1.3) was higher at younger age (<60 vs ≥60 years: 67.7% vs 61.5%; P < 0.001). In conclusion, over and beyond common risk factors, a brachial-to-central PP ratio of <1.3 is a forerunner of cardiovascular coronary complications and is an underestimated risk factor in women aged 30-60 years. Our study supports pulse wave analysis for risk stratification.
Keywords: Pulse pressure amplification, Waveform analysis, Cardiovascular risk, Population science.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Pulse pressure amplification as a hemodynamic predictor of cardiovascular disease.Hypertens Res. 2024 Nov;47(11):3270-3272. doi: 10.1038/s41440-024-01880-8. Epub 2024 Sep 11. Hypertens Res. 2024. PMID: 39261706 No abstract available.
References
-
- Benetos A, Gautier S, Labat C, Salvi P, Valbusa F, Marino F, et al. Mortality and cardiovascular events are best predicted by low central/peripheral pulse pressure amplification but not by high blood pressure levels in elderly nursing home subjects: the PARTAGE (Predictive Values of Blood Pressure and Arterial Stiffness in Institutionalized Very Aged Population) study. J Am Coll Cardiol. 2012;60:1503–11. 10.1016/j.jacc.2012.04.055 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
