

Primary diffuse large B-cell lymphoma of the central nervous system identified with CSF biomarkers
- PMID: 39039441
- PMCID: PMC11265112
- DOI: 10.1186/s12883-024-03761-6
Primary diffuse large B-cell lymphoma of the central nervous system identified with CSF biomarkers
Abstract
Background: Diagnosis of primary diffuse large B-cell lymphoma of the central nervous system (PCNSL) is challenging and often delayed. MRI imaging, CSF cytology and flow cytometry have a low sensitivity and even brain biopsies can be misleading. We report three cases of PCNSL with various clinical presentation and radiological findings where the diagnosis was suggested by novel CSF biomarkers and subsequently confirmed by brain biopsy or autopsy.
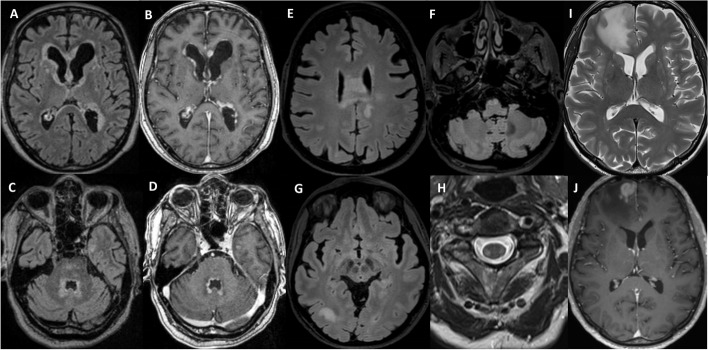
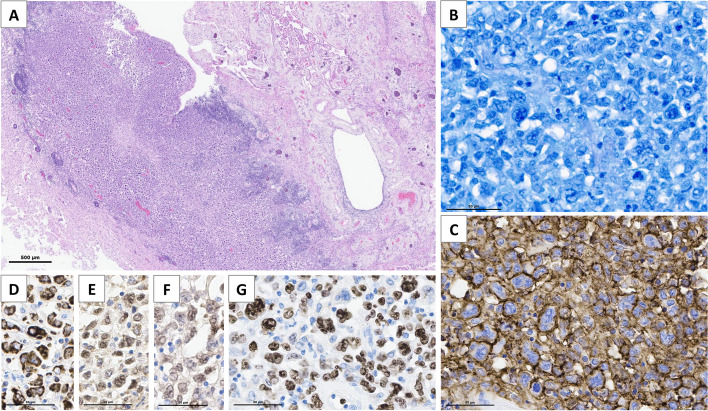
Case presentations: The first case is a 79-year-old man with severe neurocognitive dysfunction and static ataxia evolving over 5 months. Brain MRI revealed a nodular ventriculitis. An open brain biopsy was inconclusive. The second case is a 60-year-old woman with progressive sensory symptoms in all four limbs, evolving over 1 year. Brain and spinal MRI revealed asymmetric T2 hyperintensities of the corpus callosum, corona radiata and corticospinal tracts. The third case is a 72-year-old man recently diagnosed with primary vitreoretinal lymphoma of the right eye. A follow-up brain MRI performed 4 months after symptom onset revealed a T2 hyperintense fronto-sagittal lesion, with gadolinium uptake and perilesional edema. In all three cases, CSF flow cytometry and cytology were negative. Mutation analysis on the CSF (either by digital PCR or by next generation sequencing) identified the MYD88 L265P hotspot mutation in all three cases. A B-cell clonality study, performed in case 1 and 2, identified a monoclonal rearrangement of the immunoglobulin light chain lambda (IGL) and kappa (IGK) gene. CSF CXCL-13 and IL-10 levels were high in all three cases, and IL-10/IL-6 ratio was high in two. Diagnosis of PCNSL was later confirmed by autopsy in case 1, and by brain biopsy in case 2 and 3.
Conclusions: Taken together, 5 CSF biomarkers (IL-10, IL-10/IL-6 ratio, CXCL13, MYD88 mutation and monoclonal IG gene rearrangements) were strongly indicative of a PCNSL. Using innovative CSF biomarkers can be sensitive and complementary to traditional CSF analysis and brain biopsy in the diagnosis of PCNSL, potentially allowing for earlier diagnosis and treatment.
Keywords: Biomarker; Cerebrospinal fluid; Lymphoma; PCNSL.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
