

Triglyceride glucose index as a predictor for non-alcoholic fatty liver disease: insights from a longitudinal analysis in non-obese individuals
- PMID: 39040897
- PMCID: PMC11260781
- DOI: 10.3389/fmed.2024.1429413
Triglyceride glucose index as a predictor for non-alcoholic fatty liver disease: insights from a longitudinal analysis in non-obese individuals
Abstract
Background: A substantial portion of non-obese population is afflicted with Non-alcoholic Fatty Liver Disease (NAFLD). The Triglyceride Glucose (TyG) index, a quantifier of insulin resistance magnitude, is determined by the product of fasting plasma glucose and triglyceride concentrations. The relationship between the TyG index and NAFLD within this cohort remains ambiguous.
Methods: We conducted a retrospective analysis utilizing datasets acquired from the Dryad digital repository. Non-obese participants (BMI < 25 kg/m2) were enrolled at the Wenzhou Medical Center of Wenzhou People's Hospital between January 2010 and December 2014. Demographic information and biochemical parameters were systematically compiled, and the diagnosis of NAFLD was established through ultrasonographic evidence.
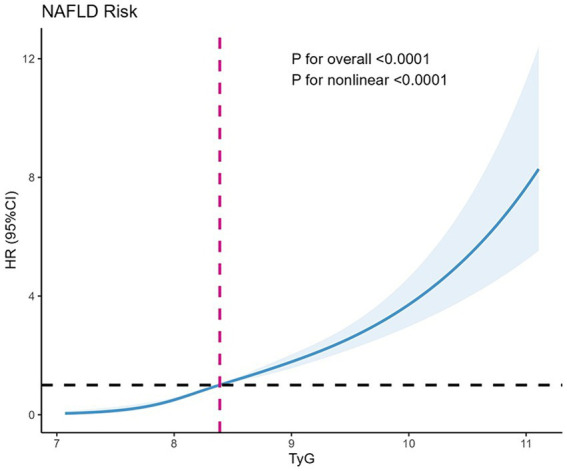
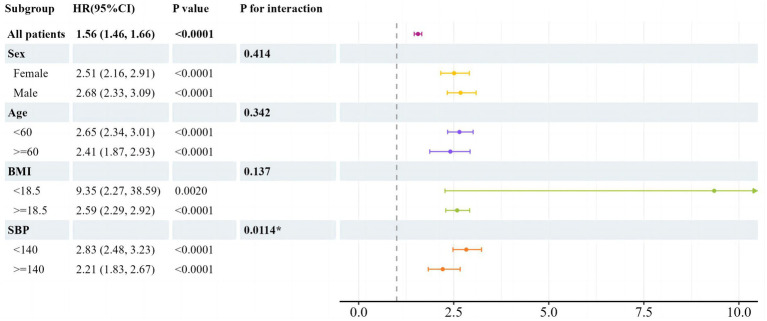
Results: This study cohort included 16,172 non-obese participants with a 5-year follow-up, among whom 2,322 (14.36%) developed NAFLD. The disparity between TyG index quartiles in the accumulative incidence of new-onset NAFLD was distinct, with an increasing risk of new-onset NAFLD as the TyG index increased. Participants in highest quartile exhibited the maximum risk of NAFLD. In the fully adjusted model 3, the hazard ratios for NAFLD in Q2, Q3, and Q4 were 2.15 (1.62, 2.87), 2.89 (2.20, 3.80) and 4.58 (3.48, 6.02), respectively. Meanwhile, the TyG index and NAFLD risk showed a highly significant overall correlation (p < 0.0001) and nonlinearity (p < 0.0001) according to the limited cubic splines. In subgroup analysis, a significant interaction was noted between new-onset NAFLD and SBP (<140 mmHg vs. ≥140 mmHg; P for interaction = 0.0114). The SBP < 140 mmHg subgroup demonstrated an enhanced TyG index influence on NAFLD risk (HR = 2.83, 95% CI: 2.48-3.23, p < 0.0001).
Conclusion: The TyG index serves as a straightforward instrument for assessing NAFLD risk in non-obese individuals, enabling prompt identification and management in this population segment.
Keywords: NAFLD; fatty liver index; non-obese population; nonalcoholic fatty liver disease; triglyceride glucose index.
Copyright © 2024 Ning, Zheng, Yan and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
[Triglyceride-glucose index in non-obese individuals: its association with and predictive value for non-alcoholic fatty liver disease].Nan Fang Yi Ke Da Xue Xue Bao. 2024 Jul 20;44(7):1266-1271. doi: 10.12122/j.issn.1673-4254.2024.07.06. Nan Fang Yi Ke Da Xue Xue Bao. 2024. PMID: 39051072 Free PMC article. Chinese.
-
Association between triglyceride glucose-body mass index and non-alcoholic fatty liver disease in the non-obese Chinese population with normal blood lipid levels: a secondary analysis based on a prospective cohort study.Lipids Health Dis. 2020 Oct 28;19(1):229. doi: 10.1186/s12944-020-01409-1. Lipids Health Dis. 2020. PMID: 33109219 Free PMC article.
-
Baseline level and change trajectory of the triglyceride-glucose index in relation to the development of NAFLD: a large population-based cohort study.Front Endocrinol (Lausanne). 2023 May 8;14:1137098. doi: 10.3389/fendo.2023.1137098. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37223043 Free PMC article.
-
Association between the atherogenic index of plasma and new-onset non-alcoholic fatty liver disease in non-obese participants.Front Endocrinol (Lausanne). 2022 Aug 18;13:969783. doi: 10.3389/fendo.2022.969783. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36060971 Free PMC article.
-
The triglyceride and glucose index and risk of nonalcoholic fatty liver disease: A dose-response meta-analysis.Front Endocrinol (Lausanne). 2023 Jan 19;13:1043169. doi: 10.3389/fendo.2022.1043169. eCollection 2022. Front Endocrinol (Lausanne). 2023. PMID: 36743937 Free PMC article.
Cited by
-
Correlation between hs-CRP-triglyceride glucose index and NAFLD and liver fibrosis.BMC Gastroenterol. 2025 Apr 12;25(1):252. doi: 10.1186/s12876-025-03870-7. BMC Gastroenterol. 2025. PMID: 40221654 Free PMC article.
-
Comparison of the predictive value of TyG index and METS-IR for OSA combined with NAFLD: a retrospective observational study based on a physical examination population.BMC Gastroenterol. 2025 Apr 21;25(1):279. doi: 10.1186/s12876-025-03856-5. BMC Gastroenterol. 2025. PMID: 40259241 Free PMC article.
-
Association between TyG-related parameters and NAFLD risk in Japanese non-obese population.Sci Rep. 2025 Feb 28;15(1):7119. doi: 10.1038/s41598-025-88478-3. Sci Rep. 2025. PMID: 40016248 Free PMC article.
-
Modified triglyceride-glucose indices as novel predictors of metabolic dysfunction-associated fatty liver disease in US adolescents: a nationally representative study from NHANES 2017-2020.BMC Gastroenterol. 2025 May 1;25(1):325. doi: 10.1186/s12876-025-03915-x. BMC Gastroenterol. 2025. PMID: 40312305 Free PMC article.
-
Triglyceride-glucose index associated with anthropometric parameters: Early markers in the progression of nonalcoholic fatty liver disease.Hepatol Forum. 2025 Jul 7;6(3):137-138. doi: 10.14744/hf.2025.2025.0005. eCollection 2025. Hepatol Forum. 2025. PMID: 40686593 Free PMC article. No abstract available.
References
Associated data
LinkOut - more resources
Full Text Sources