

Can plethysmographic capillary refill time predict lactate during sepsis? An observational study from Morocco
- PMID: 39040945
- PMCID: PMC11261390
- DOI: 10.1016/j.afjem.2024.06.007
Can plethysmographic capillary refill time predict lactate during sepsis? An observational study from Morocco
Abstract
Introduction: Blood lactate is a marker of tissue hypoxia while capillary refill time (CRT) is a surrogate of tissue perfusion. Measuring these parameters is recommended for assessing circulatory status and guiding resuscitation. However, blood lactate is not widely available in African emergency departments. Additionally, CRT assessment faces challenges related to its precision and reproducibility. This study aims to evaluate the accuracy of visual CRT(V-CRT) compared to plethysmographic CRT (P-CRT) in predicting lactate levels among septic patients.
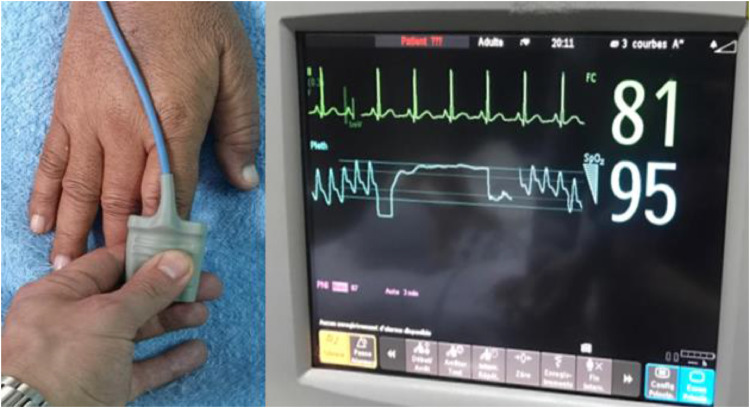
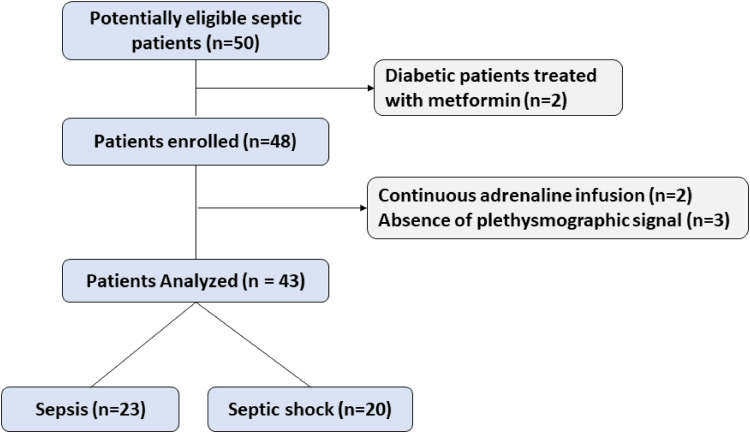
Methods: This prospective observational study enrolled consecutive patients with sepsis or septic shock over a 6-month period from a tertiary hospital in Marrakech, Morroco. V-CRT and P-CRT were evaluated upon admission, and simultaneous measurements of arterial lactate levels were obtained. The precision of V-CRT and P-CRT in predicting arterial lactate was assessed using ROC curve analysis.
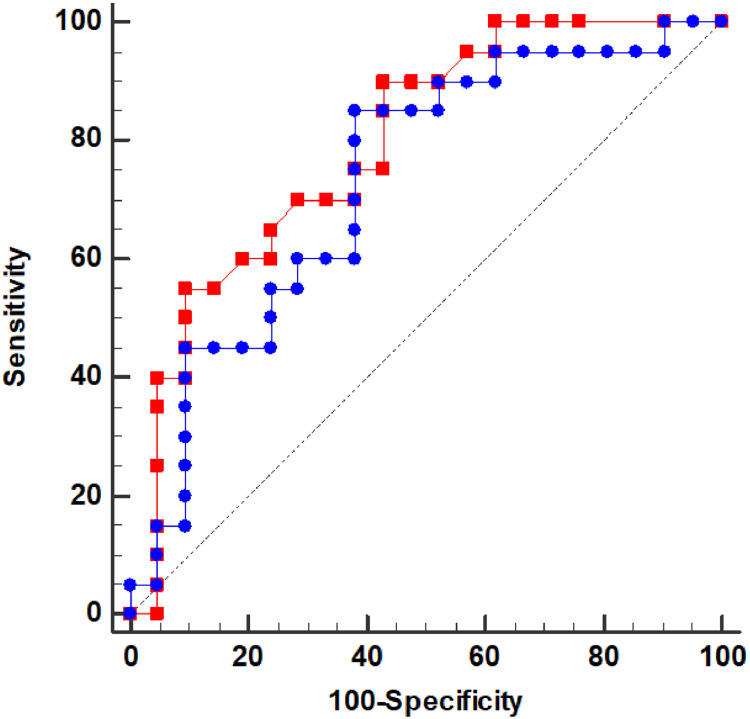
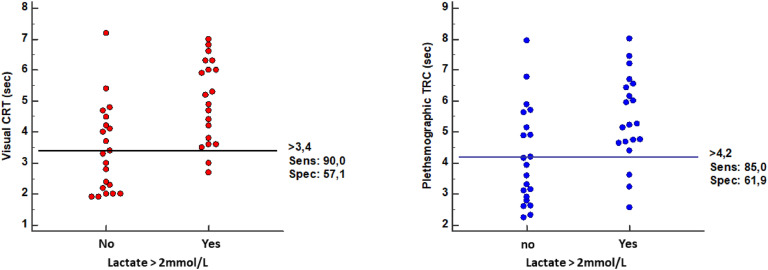
Results: Forty-three patients aged of 64±15 years, of whom 70 % were male, were included in the study. Of these, 23 patients (53 %) had sepsis, and 20 patients (47 %) experienced septic shock. Both V-CRT and P-CRT demonstrated statistically significant correlations with arterial lactate, with correlation coefficients of 0.529 (p < 0.0001) and 0.517 (p = 0.001), respectively. ROC curve analysis revealed that V-CRT exhibited satisfactory accuracy in predicting arterial lactate levels >2 mmol/l, with an area under the curve (AUC) of 0.8 (95 % CI=0.65 - 0.93; p < 0.0001). The prediction ability of P-CRT was lower than V-CRT with an AUC of 0.73 (95 % CI: 0.57-0.89; p = 0.043). The optimal thresholds were determined as 3.4 s for V-CRT (sensitivity = 90 %, specificity = 58 %) and 4.1 s for P-CRT (sensitivity = 85 %, specificity = 62 %).
Conclusion: These findings suggest that the plethysmographic evaluation did not improve the accuracy of CRT for predicting lactate level. However, V-CRT may still serve as a viable surrogate for lactate in septic patients in low-income settings.
Keywords: Capillary refill time; Lactate; Low-income setting; Plethysmography; Sepsis; Septic shock.
© 2024 The Authors. Published by Elsevier B.V. on behalf of African Federation for Emergency Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
