

Enzymatic Modulation of the Pulmonary Glycocalyx Enhances Susceptibility to Streptococcus pneumoniae
- PMID: 39042016
- PMCID: PMC11622634
- DOI: 10.1165/rcmb.2024-0003OC
Enzymatic Modulation of the Pulmonary Glycocalyx Enhances Susceptibility to Streptococcus pneumoniae
Abstract
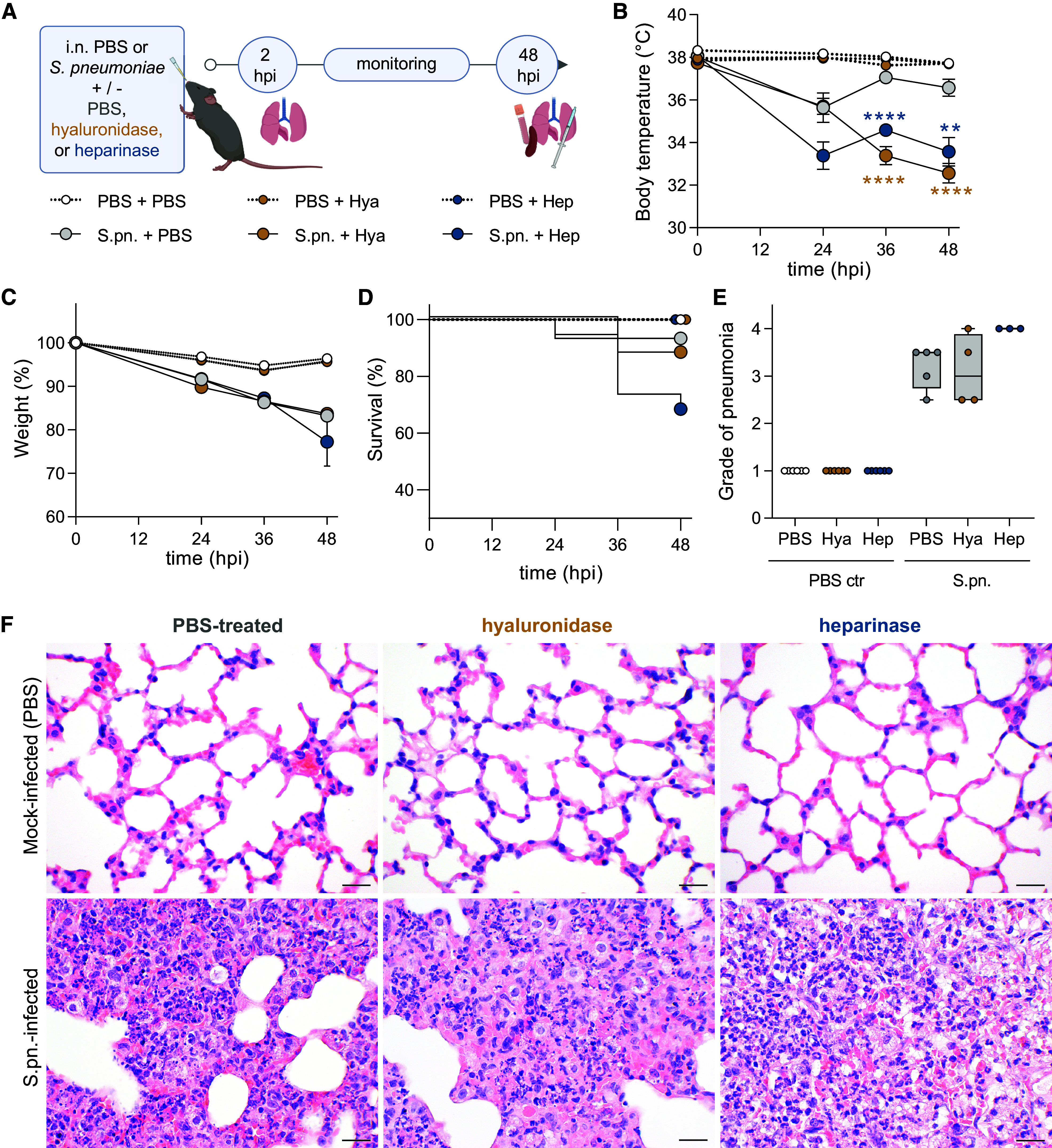
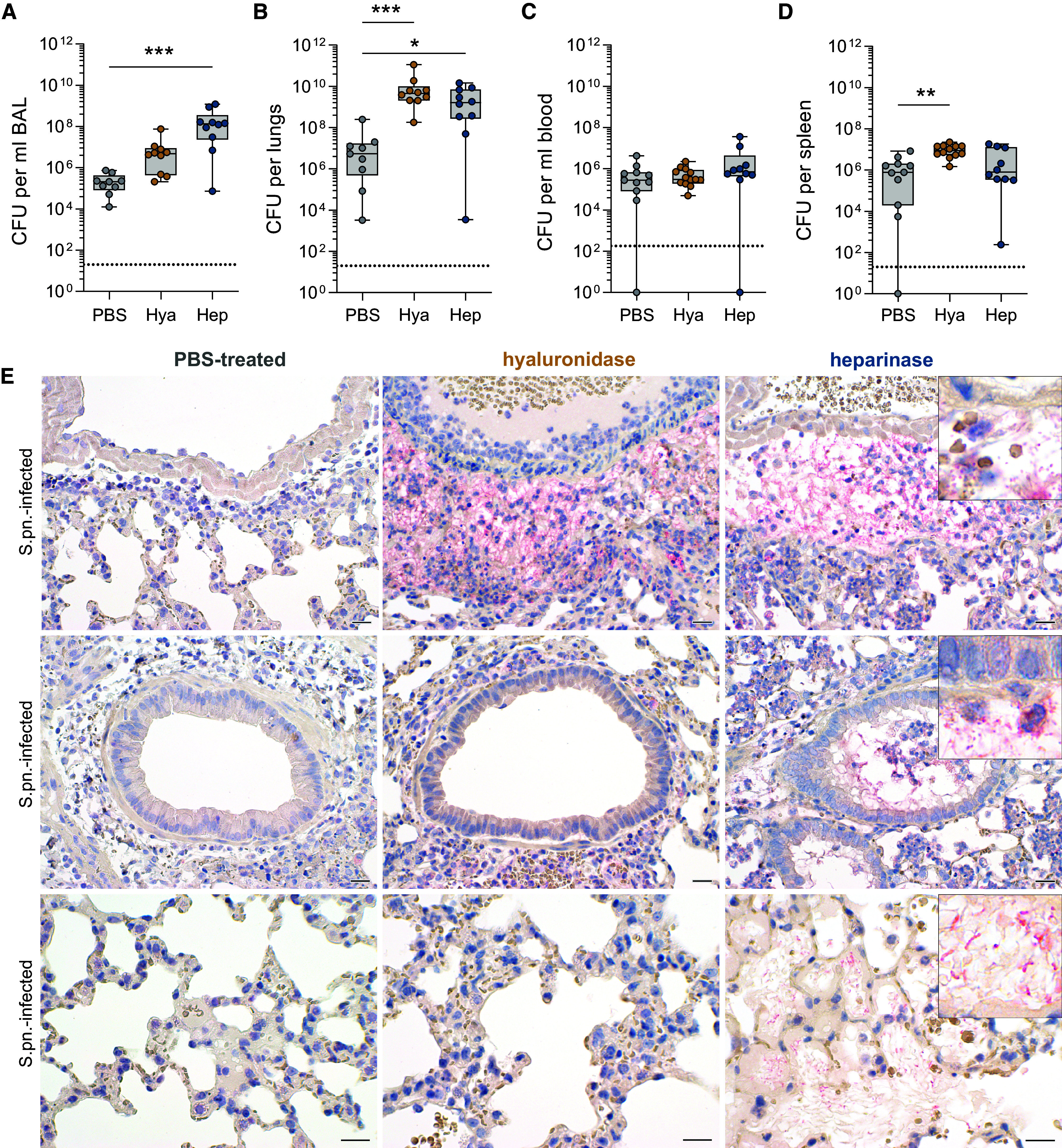
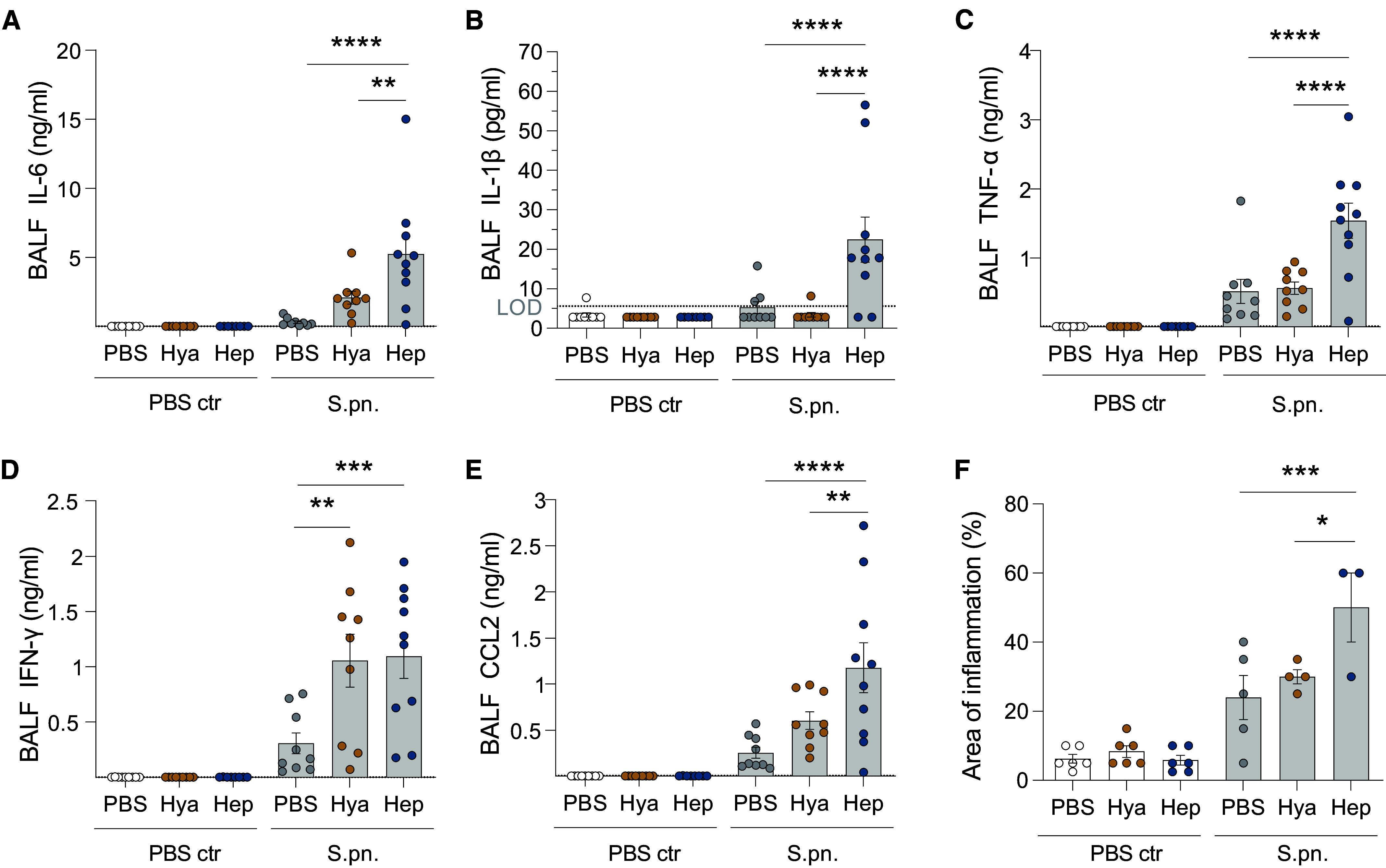
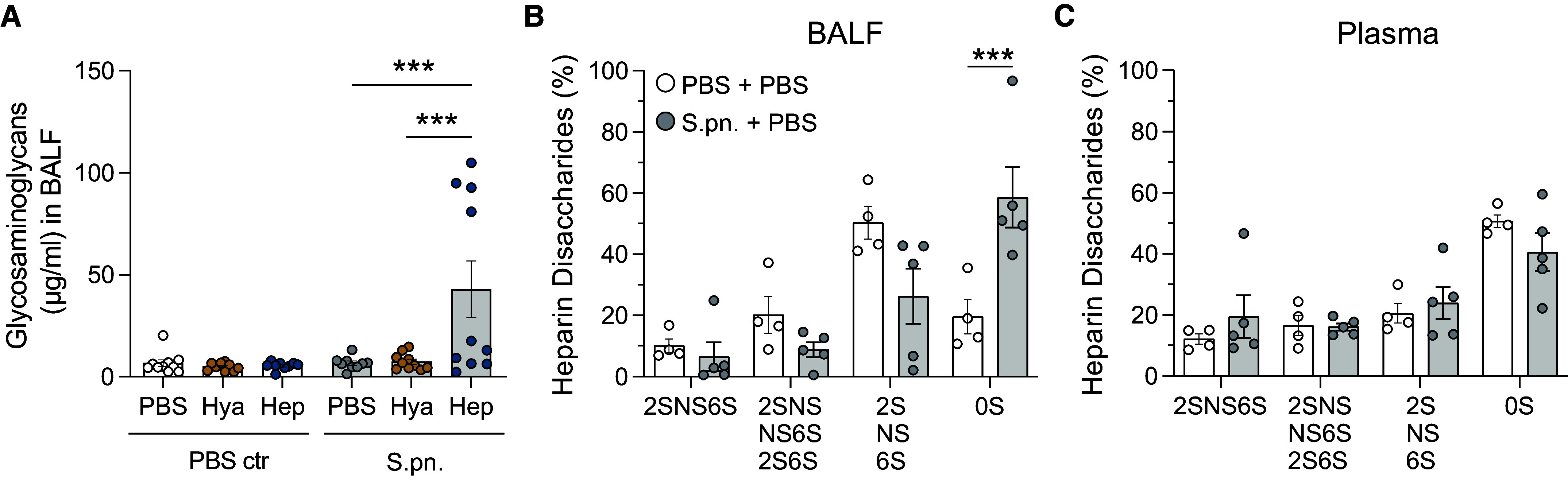
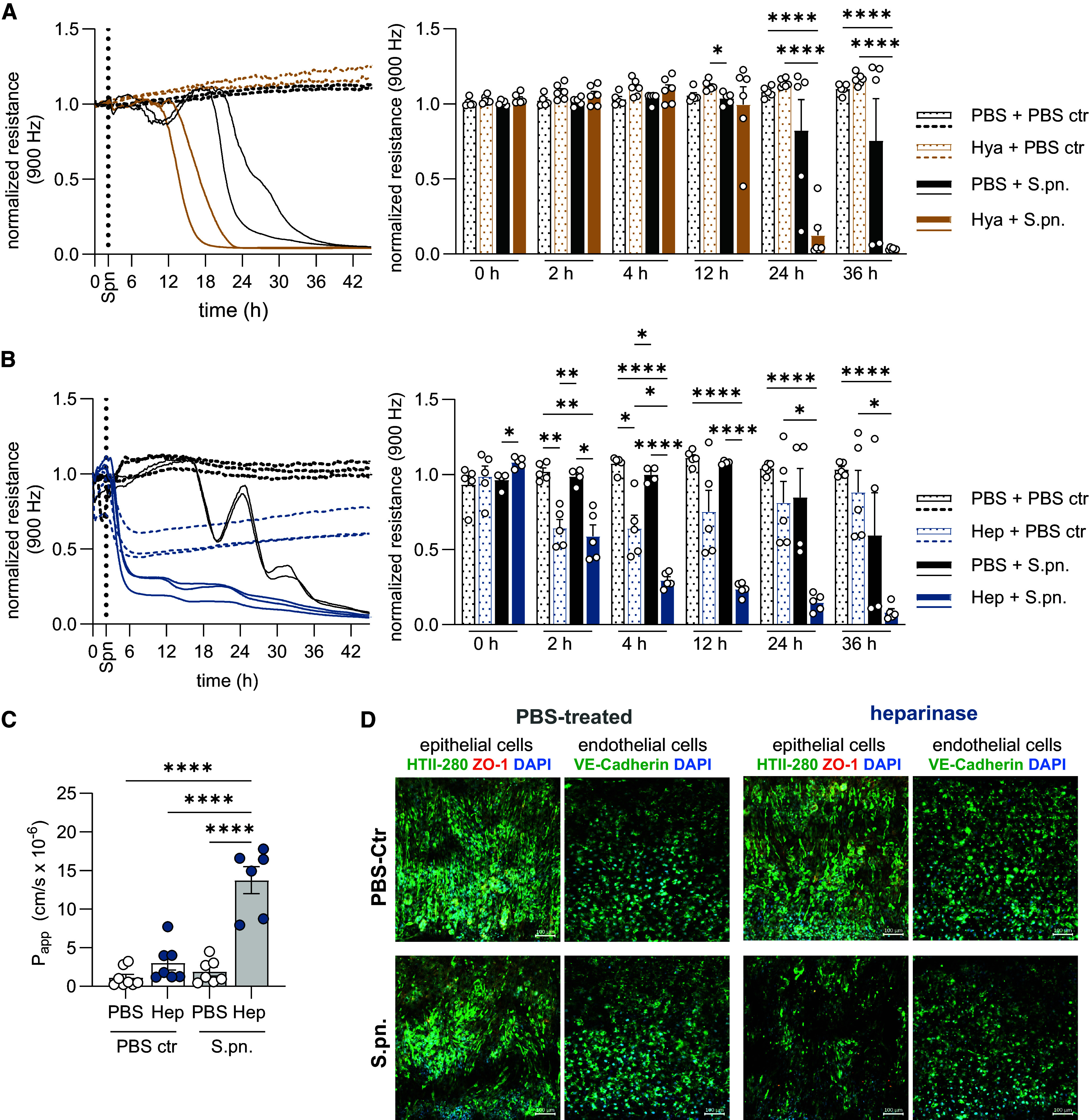
The pulmonary epithelial glycocalyx is rich in glycosaminoglycans such as hyaluronan and heparan sulfate. Despite their presence, the importance of these glycosaminoglycans in bacterial lung infections remains elusive. To address this, we intranasally inoculated mice with Streptococcus pneumoniae in the presence or absence of enzymes targeting pulmonary hyaluronan and heparan sulfate, followed by characterization of subsequent disease pathology, pulmonary inflammation, and lung barrier dysfunction. Enzymatic degradation of hyaluronan and heparan sulfate exacerbated pneumonia in mice, as evidenced by increased disease scores and alveolar neutrophil recruitment. However, targeting epithelial hyaluronan in combination with S. pneumoniae infection further exacerbated systemic disease, indicated by elevated splenic bacterial load and plasma concentrations of proinflammatory cytokines. In contrast, enzymatic cleavage of heparan sulfate resulted in increased bronchoalveolar bacterial burden, lung damage, and pulmonary inflammation in mice infected with S. pneumoniae. Accordingly, heparinase-treated mice also exhibited disrupted lung barrier integrity as evidenced by higher alveolar edema scores and vascular protein leakage into the airways. This finding was corroborated in a human alveolus-on-a-chip platform, confirming that heparinase treatment also disrupts the human lung barrier during S. pneumoniae infection. Notably, enzymatic pretreatment with either hyaluronidase or heparinase also rendered human epithelial cells more sensitive to pneumococci-induced barrier disruption, as determined by transepithelial electrical resistance measurements, consistent with our findings in murine pneumonia. Taken together, these findings demonstrate the importance of intact hyaluronan and heparan sulfate in limiting pneumococci-induced damage, pulmonary inflammation, and epithelial barrier function and integrity.
Keywords: acute lung injury; community-acquired pneumonia; glycosaminoglycans; heparan sulfate; hyaluronan.
Figures


Comment in
-
Respiratory Epithelial Cell Surface Decoration Provides Defense against Bacterial Damage during Infection.Am J Respir Cell Mol Biol. 2024 Dec;71(6):625-627. doi: 10.1165/rcmb.2024-0306ED. Am J Respir Cell Mol Biol. 2024. PMID: 39051864 Free PMC article. No abstract available.
References
-
- Welte T, Torres A, Nathwani D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax . 2012;67:71–79. - PubMed
-
- Howard LS, Sillis M, Pasteur MC, Kamath AV, Harrison BD. Microbiological profile of community-acquired pneumonia in adults over the last 20 years. J Infect . 2005;50:107–113. - PubMed
-
- Ewig S, Woodhead M, Torres A. Towards a sensible comprehension of severe community-acquired pneumonia. Intensive Care Med . 2011;37:214–223. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
