

A randomized, pilot trial comparing vaginal hyaluronic acid to vaginal estrogen for the treatment of genitourinary syndrome of menopause
- PMID: 39042017
- PMCID: PMC11469619
- DOI: 10.1097/GME.0000000000002390
A randomized, pilot trial comparing vaginal hyaluronic acid to vaginal estrogen for the treatment of genitourinary syndrome of menopause
Abstract
Objective: The aim of this study was to compare the efficacy of a non-hormone alternative, vaginal hyaluronic acid (HLA), to a standard-of-care therapy, vaginal estrogen, for the treatment of genitourinary syndrome of menopause (GSM).
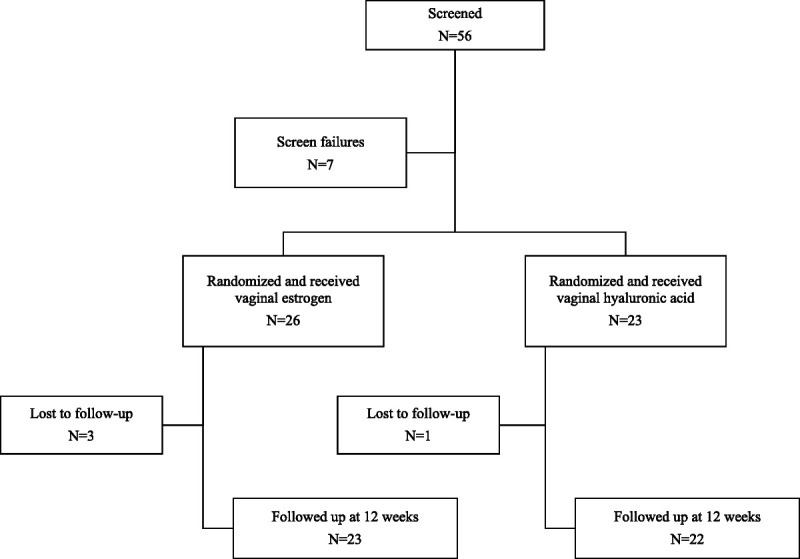
Methods: This was a randomized, parallel arm pilot trial. Women with GSM were randomized to an HLA vaginal suppository or vaginal estrogen cream for 12 wk to compare the primary outcome, the vulvovaginal symptom questionnaire (VSQ) score. Secondary outcomes included the following: the female sexual function index (FSFI), the vaginal symptom index (VSI), visual analog scale (VAS) for dyspareunia, vaginal itching, and vaginal dryness, patient global impression of improvement (PGI-I) at follow-up, vaginal maturation index, and vaginal pH. Differences between treatment groups were estimated using the two-sided, two-sample t -test and 95% confidence intervals.
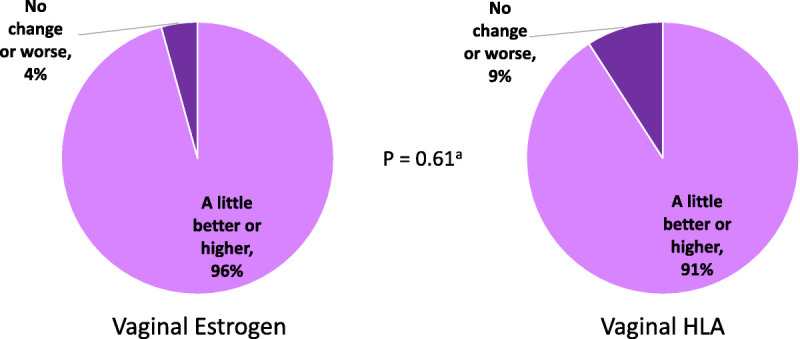
Results: Forty-nine women were randomized and 45 participants (vaginal estrogen = 23, vaginal HLA = 22) provided data at week 12. Baseline characteristics were similar in both groups. On the VSQ, there was no observed difference in overall scores between the HLA and vaginal estrogen groups at 12 wk ( P = 0.81). Improvement was seen within both treatment groups on the VSQ after 12 wk. The VAS score, total VSI score, total FSFI score, and vaginal pH improved over time; however, improvement did not differ between study arms. Over 90% participants noted improvement on the PGI-I in both groups ( P = 0.61). No treatment-related serious adverse events occurred.
Conclusions: There were no clinically meaningful differences between vaginal HLA and vaginal estrogen for the treatment of GSM after 12 wk. Vaginal HLA may be a promising non-hormone therapy for GSM.
Trial registration: ClinicalTrials.gov NCT04544475.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The Menopause Society.
Conflict of interest statement
Financial disclosure/conflicts of interest: Benjamin M. Brucker is an investigator, speaker, and advisor for AbbVie; advisor for Watkins Conti; investigator, speaker, and advisor for Urovant; advisor for Palette, funding from Myovant, ProPharma, Axonics, and Medtronic. Erinn M. Hale receives institutional funding from the National Institutes of Health, PCORI, and Educational Foundation of America, and is an editor for Reproductive, Female and Child Health Journal. Lila Nachtigall is chairman of the board of the Foundation for Woman's Wellness, which is a non-profit for which she receives no compensation. Christina Escobar receives institutional funding from Watkins Conti products. The other authors have nothing to disclose.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
