

Polyp size measurement during colonoscopy using a virtual scale: variability and systematic differences
- PMID: 39043201
- PMCID: PMC11774581
- DOI: 10.1055/a-2371-3693
Polyp size measurement during colonoscopy using a virtual scale: variability and systematic differences
Abstract
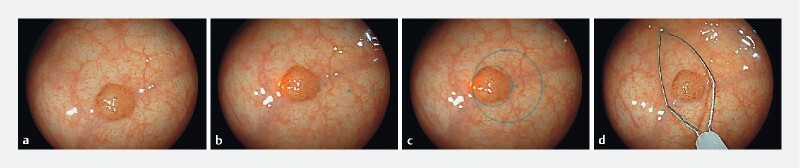
BACKGROUND : Accurate polyp size measurement is important for polyp risk stratification and decision-making regarding polypectomy and surveillance. Recently, a virtual scale (VS) function has been developed that allows polyp size measurement through projection of an adaptive VS onto colorectal polyps during real-time endoscopy. We aimed to evaluate the VS in terms of variability and systematic differences. METHODS : We conducted a video-based study with 120 colorectal polyps, measured by eight dedicated colorectal gastroenterologists (experts) and nine gastroenterology residents following endoscopy training (trainees). Three endoscopic measurement methods were compared: (1) visual, (2) snare and (3) VS measurement. We evaluated the method-specific variance (as measure of variability) in polyp size measurements and systematic differences between these methods. RESULTS : Variance in polyp size measurements was significantly lower for VS measurements compared to visual and snare measurements for both experts (0.52 vs. 1.59 and 1.96, p < 0.001) and trainees (0.59 vs. 2.21 and 2.53, p < 0.001). VS measurement resulted in a higher percentage of polyps assigned to the same size category by all endoscopists compared to visual and snare measurements (experts: 69 % vs. 55 % and 59 %; trainees: 67 % vs. 51 % and 47 %) and reduced the maximum difference between individual endoscopists regarding the percentage of polyps assigned to the ≥ 10 mm size category (experts: 1.7 % vs. 10.0 % and 5.0 %; trainees: 2.5 % vs. 6.7 % and 11.7 %). Systematic differences between methods were < 0.5 mm. CONCLUSIONS : Use of the VS leads to lower polyp size measurement variability and more uniform polyp sizing by individual endoscopists compared to visual and snare measurements.
Trial registration: ClinicalTrials.gov NCT05499546.
This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
H. Beaumont has received speaker fees from Medtronic. B. Bastiaansen has received speaker fees from Olympus, Tillotts Pharma AG, and Ovesco Endoscopy AG. D. Ramsoekh has received a research grant from AbbVie (outside the submitted work) and served as a member of the Data Safety Monitoring Board of Vivoryon Therapeutics. P. Fockens has received research support from Boston Scientific and a consulting fee from Olympus and Cook Endoscopy. E. Dekker received a research grant from Fujifilm, honoraria for consultancy from Olympus, Fujifilm, Ambu, InterVenn, Norgine, and Exact Sciences and speakers' fees from Olympus, GI Supply, Norgine, IPSEN/Mayoly, FujiFilm and Steris. The remaining authors declare that they have no conflict of interest.
Figures



References
-
- Hassan C, Pickhardt P J, Kim D H et al. Systematic review: distribution of advanced neoplasia according to polyp size at screening colonoscopy. Aliment Pharmacol Ther. 2010;31:210–217. - PubMed
-
- Hassan C, Antonelli G, Dumonceau J M et al. Post-polypectomy colonoscopy surveillance: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – update 2020. Endoscopy. 2020;52:687–700. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical