

Comprehensive analysis of endoplasmic reticulum stress related signature in head and neck squamous carcinoma
- PMID: 39043683
- PMCID: PMC11266686
- DOI: 10.1038/s41598-024-65090-5
Comprehensive analysis of endoplasmic reticulum stress related signature in head and neck squamous carcinoma
Abstract
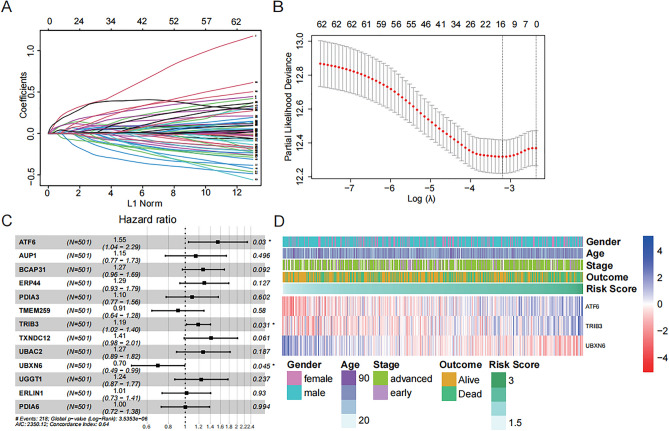
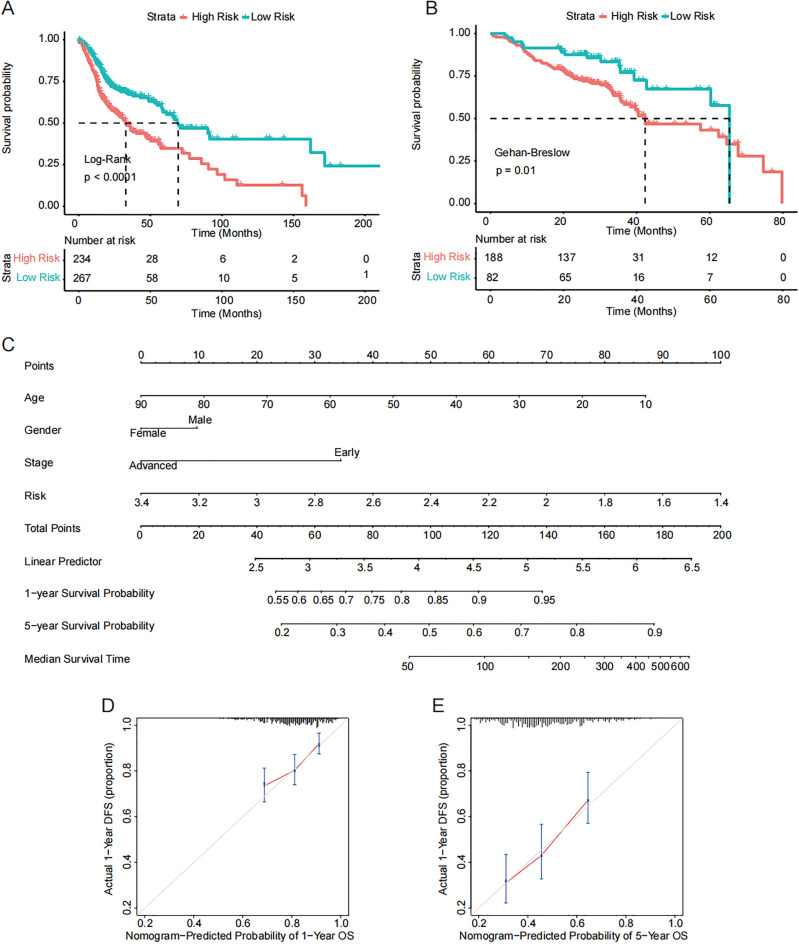
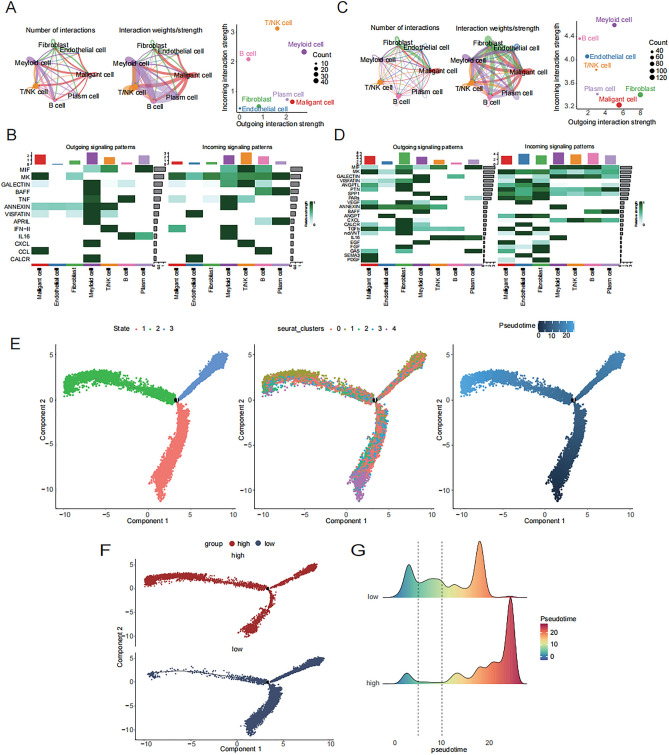
Head and neck squamous carcinoma (HNSC) is a prevalent malignant disease, with the majority of patients being diagnosed at an advanced stage. Endoplasmic reticulum stress (ERS) is considered to be a process that promotes tumorigenesis and impacts the tumor microenvironment (TME) in various cancers. The study aims to investigate the predictive value of ERS in HNSC and explore the correlation between ERS-related genes and TME. A series of bioinformatics analyses were carried out based on mRNA and scRNA-seq data from the TCGA and GEO databases. We conducted RT-qPCR and western blot to validate the signature, and performed cell functional experiments to investigate the in vitro biological functions of the gene. We identified 63 ERS-related genes that were associated with outcome and stage in HNSC. A three-gene signature (ATF6, TRIB3, and UBXN6) was developed, which presents predictive value in the prognosis and immunotherapy response of HNSC patients. The high-risk group exhibited a worse prognosis but may benefit from immunotherapy. Furthermore, there was a significant correlation between the signature and immune infiltration. In the high-risk group, fibroblasts were more active in intercellular communication, and more T cells were observed at the end of the sequential phase. The genes in the ERS-related signature were overexpressed in HNSC cells, and the knockdown of TRIB3 significantly inhibited cell proliferation and migration. This study established a novel ERS-related signature that has potential implications for HNSC therapy and the understanding of TME.
Keywords: Endoplasmic reticulum stress; Head and neck squamous carcinoma; Immunotherapy response; Prognosis; TME.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
