

A multi-step approach to overcome challenges in the management of head and neck lymphatic malformations, and response to treatment
- PMID: 39044220
- PMCID: PMC11265367
- DOI: 10.1186/s13023-024-03200-2
A multi-step approach to overcome challenges in the management of head and neck lymphatic malformations, and response to treatment
Abstract
Background: Lymphatic malformations are vascular developmental anomalies varying from local superficial masses to diffuse infiltrating lesions, resulting in disfigurement. Patients' outcomes range from spontaneous regression to severe sequelae notwithstanding appropriate treatment. The current classification guides, in part, clinicians through the decision-making process, prognosis prediction and choice of therapeutic strategies. Even though the understanding of molecular basis of the disease has been recently improved, a standardized management algorithm has not been reached yet.
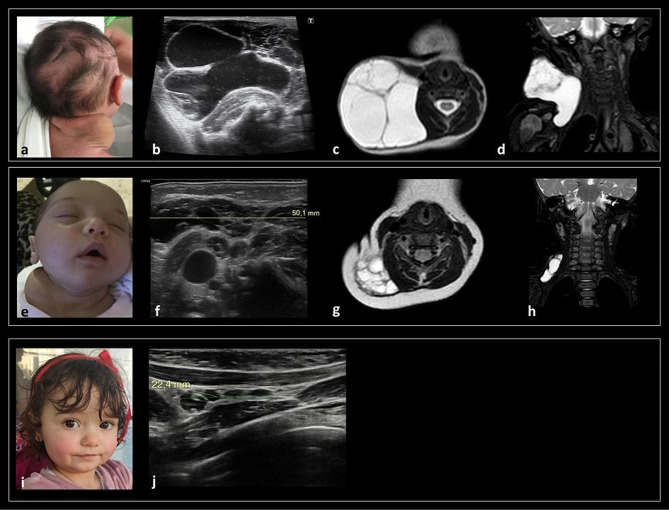
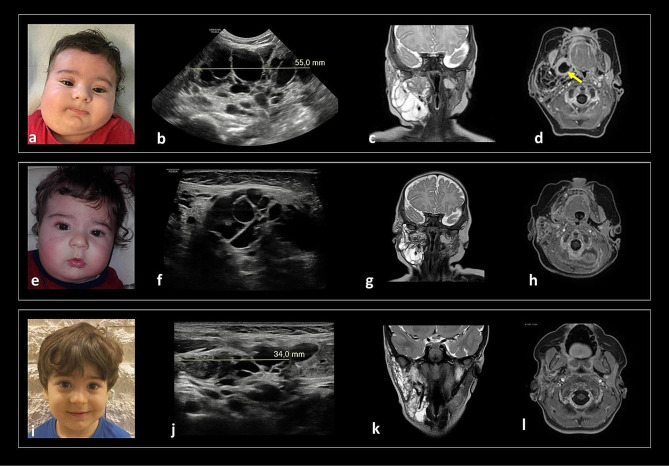
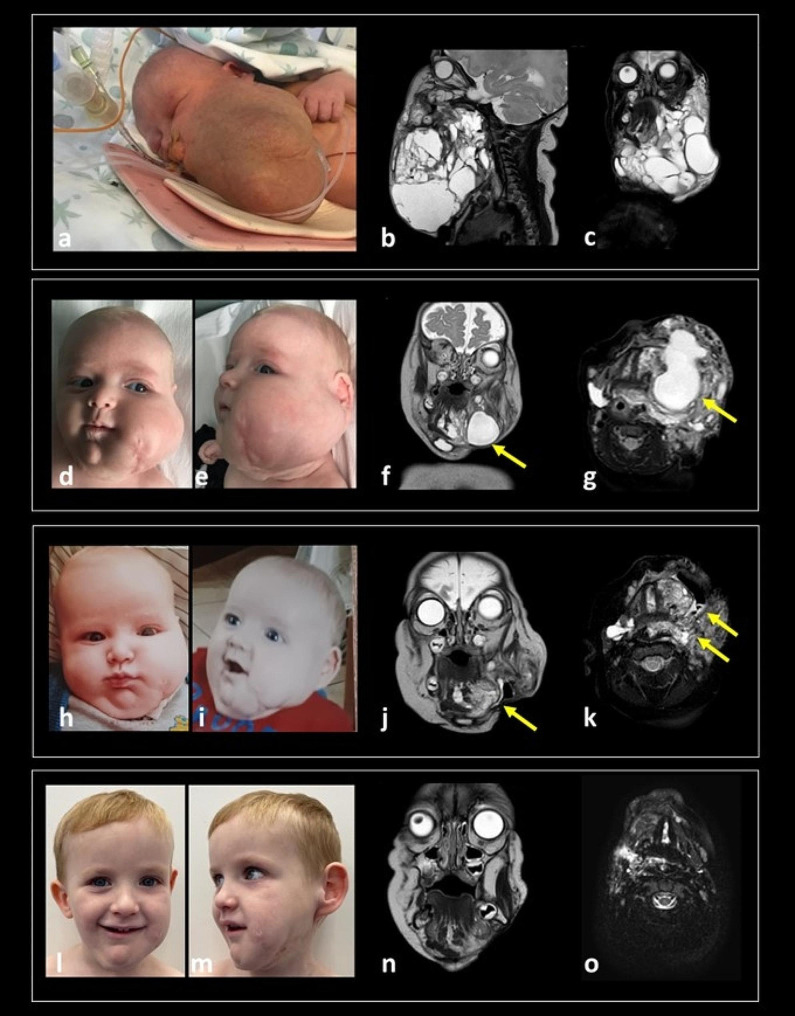
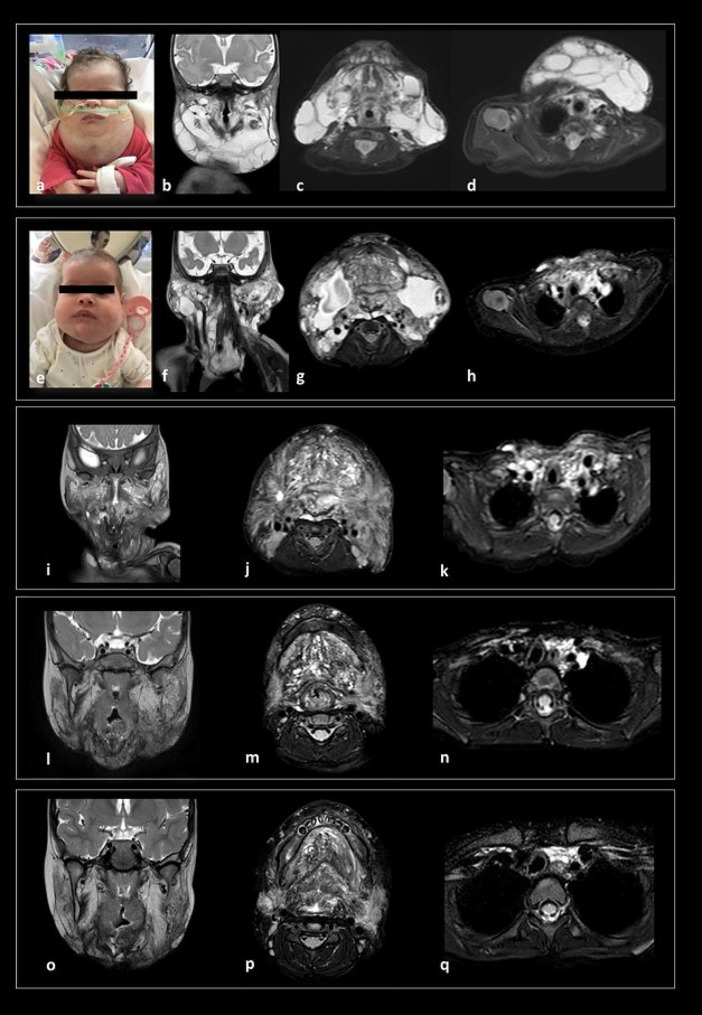
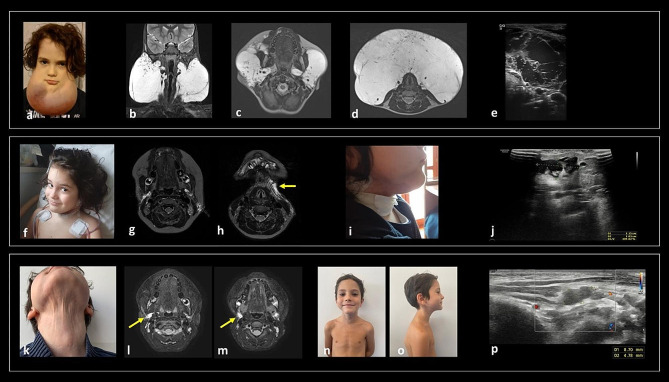
Results: Here, we report our experience on five children with different lymphatic anomalies of the head and neck region treated by applying a multidisciplinary approach reaching a consensus among specialists on problem-solving and setting priorities.
Conclusions: Although restitutio ad integrum was rarely achieved and the burden of care is challenging for patients, caregivers and healthcare providers, this study demonstrates how the referral to expert centres can significantly improve outcomes by alleviating parental stress and ameliorating patients' quality of life. A flow-chart is proposed to guide the multidisciplinary care of children with LMs and to encourage multidisciplinary collaborative initiatives to implement dedicated patients' pathways.
Keywords: Alpelisib; Lymphangioma; Lymphatic malformations; Personalized medicine; Sirolimus; mTOR.
© 2024. The Author(s).
Conflict of interest statement
Chiara Leoni and Nicoletta Resta belong to the advisory board for PROS by Novartis. The other authors declare no conflict of interest.
Figures

References
-
- ISSVA classification for vascular anomalies ©.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
